正在加载图片...
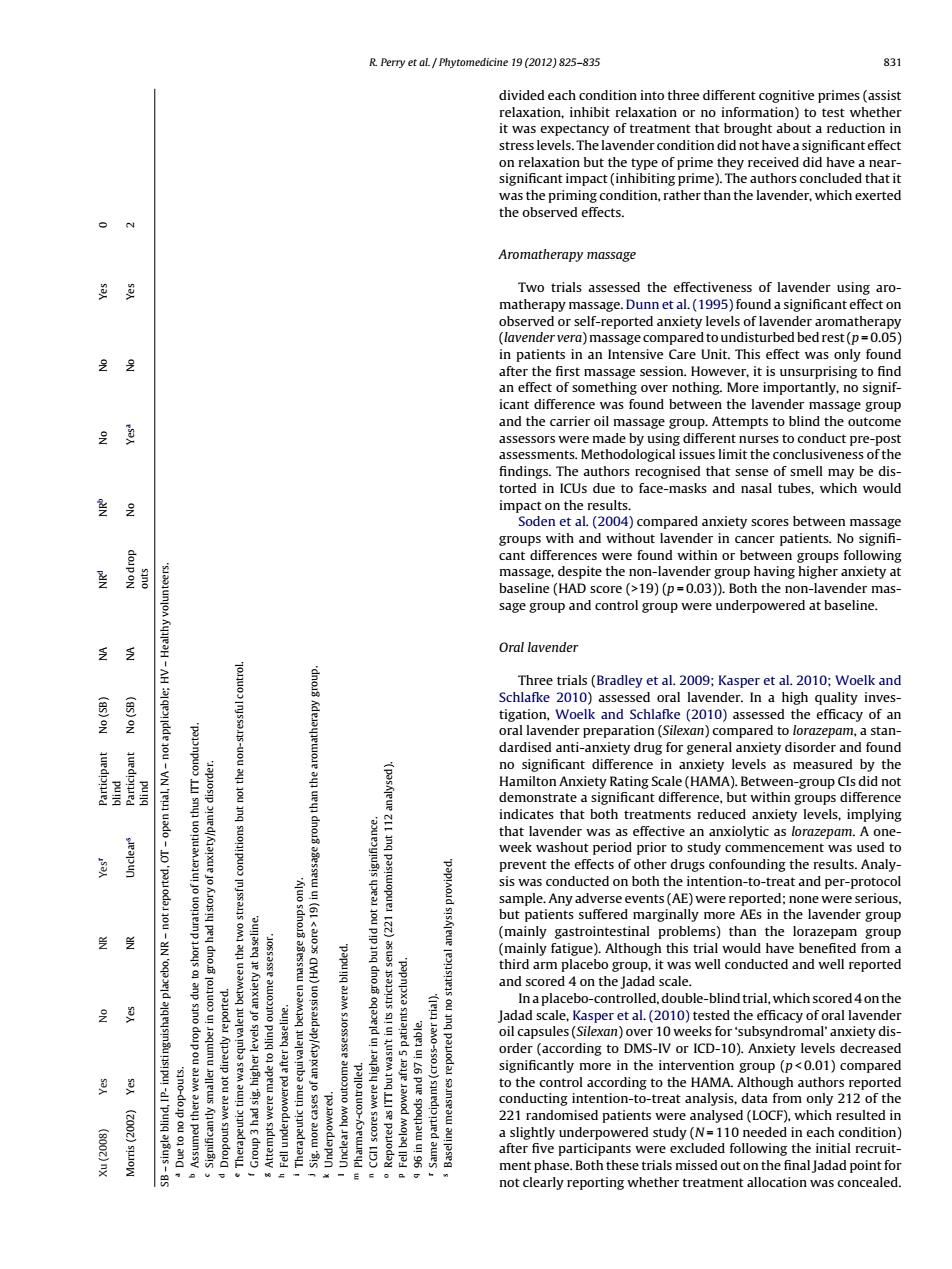
R.Perry et al Phytomedicine 19 (2012)825-835 831 divided each condition into three different cognitive primes (assist relaxation,inhibit relaxation or no information)to test whether it was expectancy of treatment that brought about a reduction in stress levels.The lavender condition did not have a significant effect on relaxation but the type of prime they received did have a near- significant impact(inhibiting prime).The authors concluded that it was the priming condition,rather than the lavender,which exerted the observed effects. Aromatherapy massage Two trials assessed the effectiveness of lavender using aro matherapy massage.Dunn et al.(1995)found a significant effect on observed or self-reported anxiety levels of lavender aromatherapy (lavender vera)massage compared to undisturbed bed rest(p=0.05) in patients in an Intensive Care Unit.This effect was only found after the first massage session.However,it is unsurprising to find an effect of something over nothing.More importantly,no signif- icant difference was found between the lavender massage group 鱼 and the carrier oil massage group.Attempts to blind the outcome assessors were made by using different nurses to conduct pre-post assessments.Methodological issues limit the conclusiveness of the findings.The authors recognised that sense of smell may be dis- torted in ICUs due to face-masks and nasal tubes,which would impact on the results. Soden et al.(2004)compared anxiety scores between massage groups with and without lavender in cancer patients.No signifi- 星 cant differences were found within or between groups following massage,despite the non-lavender group having higher anxiety at baseline (HAD score (>19)(p=0.03)).Both the non-lavender mas- sage group and control group were underpowered at baseline. Oral lavender Three trials(Bradley et al.2009;Kasper et al.2010;Woelk and Schlafke 2010)assessed oral lavender.In a high quality inves- C85)0N tigation,Woelk and Schlafke (2010)assessed the efficacy of an oral lavender preparation(Silexan)compared to lorazepam,a stan- dardised anti-anxiety drug for general anxiety disorder and found no significant difference in anxiety levels as measured by the Hamilton Anxiety Rating Scale(HAMA).Between-group Cls did not demonstrate a significant difference,but within groups difference indicates that both treatments reduced anxiety levels,implying that lavender was as effective an anxiolytic as lorazepam.A one- week washout period prior to study commencement was used to prevent the effects of other drugs confounding the results.Analy sis was conducted on both the intention-to-treat and per-protocol sample.Any adverse events(AE)were reported;none were serious but patients suffered marginally more AEs in the lavender group (mainly gastrointestinal problems)than the lorazepam group (mainly fatigue).Although this trial would have benefited from a third arm placebo group,it was well conducted and well reported and scored 4 on the Jadad scale. In a placebo-controlled,double-blind trial,which scored 4 on the Jadad scale,Kasper et al.(2010)tested the efficacy of oral lavender oil capsules(Silexan)over 10 weeks for'subsyndromal'anxiety dis- order (according to DMS-IV or ICD-10).Anxiety levels decreased significantly more in the intervention group (p<0.01)compared to the control according to the HAMA.Although authors reported conducting intention-to-treat analysis,data from only 212 of the 221 randomised patients were analysed (LOCF),which resulted in (8002c)nx a slightly underpowered study (N=110 needed in each condition) after five participants were excluded following the initial recruit- ment phase.Both these trials missed out on the final Jadad point for not clearly reporting whether treatment allocation was concealedR. Perry et al. / Phytomedicine 19 (2012) 825–835 831 Xu (2008) Yes No NR Yesr Participant blind No (SB) NA NRd NRb No No Yes 0 Morris (2002) Yes Yes NR Unclears Participant blind No (SB) NA No drop outs No Yesa No Yes 2 SB – single blind, IP- indistinguishable placebo, NR – not reported, OT – open trial, NA – not applicable; HV – Healthy volunteers. a Due to no drop-outs. b Assumed there were no drop outs due to short duration of intervention thus ITT conducted. c Significantly smaller number in control group had history of anxiety/panic disorder. d Dropouts were not directly reported. e Therapeutic time was equivalent between the two stressful conditions but not the non-stressful control. f Group 3 had sig. higher levels of anxiety at baseline. g Attempts were made to blind outcome assessor. h Fell underpowered after baseline. i Therapeutic time equivalent between massage groups only. j Sig. more cases of anxiety/depression (HAD score > 19) in massage group than the aromatherapy group. k Underpowered. l Unclear how outcome assessors were blinded. m Pharmacy-controlled. n CGI1 scores were higher in placebo group but did not reach significance. o Reported as ITT but wasn’t in its strictest sense (221 randomised but 112 analysed). p Fell below power after 5 patients excluded. q 96 in methods and 97 in table. r Same participants (cross-over trial). s Baseline measures reported but no statistical analysis provided. divided each condition into three different cognitive primes (assist relaxation, inhibit relaxation or no information) to test whether it was expectancy of treatment that brought about a reduction in stress levels. The lavender condition did not have a significant effect on relaxation but the type of prime they received did have a nearsignificant impact (inhibiting prime). The authors concluded that it was the priming condition, rather than the lavender, which exerted the observed effects. Aromatherapy massage Two trials assessed the effectiveness of lavender using aromatherapy massage. Dunn et al. (1995) found a significant effect on observed or self-reported anxiety levels of lavender aromatherapy (lavender vera)massage comparedtoundisturbedbedrest(p = 0.05) in patients in an Intensive Care Unit. This effect was only found after the first massage session. However, it is unsurprising to find an effect of something over nothing. More importantly, no significant difference was found between the lavender massage group and the carrier oil massage group. Attempts to blind the outcome assessors were made by using different nurses to conduct pre-post assessments. Methodological issues limit the conclusiveness of the findings. The authors recognised that sense of smell may be distorted in ICUs due to face-masks and nasal tubes, which would impact on the results. Soden et al. (2004) compared anxiety scores between massage groups with and without lavender in cancer patients. No signifi- cant differences were found within or between groups following massage, despite the non-lavender group having higher anxiety at baseline (HAD score (>19) (p = 0.03)). Both the non-lavender massage group and control group were underpowered at baseline. Oral lavender Three trials (Bradley et al. 2009; Kasper et al. 2010; Woelk and Schlafke 2010) assessed oral lavender. In a high quality investigation, Woelk and Schlafke (2010) assessed the efficacy of an oral lavender preparation (Silexan) compared to lorazepam, a standardised anti-anxiety drug for general anxiety disorder and found no significant difference in anxiety levels as measured by the Hamilton Anxiety Rating Scale (HAMA). Between-group CIs did not demonstrate a significant difference, but within groups difference indicates that both treatments reduced anxiety levels, implying that lavender was as effective an anxiolytic as lorazepam. A oneweek washout period prior to study commencement was used to prevent the effects of other drugs confounding the results. Analysis was conducted on both the intention-to-treat and per-protocol sample. Any adverse events (AE) were reported; none were serious, but patients suffered marginally more AEs in the lavender group (mainly gastrointestinal problems) than the lorazepam group (mainly fatigue). Although this trial would have benefited from a third arm placebo group, it was well conducted and well reported and scored 4 on the Jadad scale. Inaplacebo-controlled,double-blindtrial, whichscored4 onthe Jadad scale, Kasper et al. (2010) tested the efficacy of oral lavender oil capsules (Silexan) over 10 weeks for ‘subsyndromal’ anxiety disorder (according to DMS-IV or ICD-10). Anxiety levels decreased significantly more in the intervention group (p < 0.01) compared to the control according to the HAMA. Although authors reported conducting intention-to-treat analysis, data from only 212 of the 221 randomised patients were analysed (LOCF), which resulted in a slightly underpowered study (N = 110 needed in each condition) after five participants were excluded following the initial recruitment phase. Both these trials missed out on the final Jadad pointfor not clearly reporting whether treatment allocation was concealed