正在加载图片...
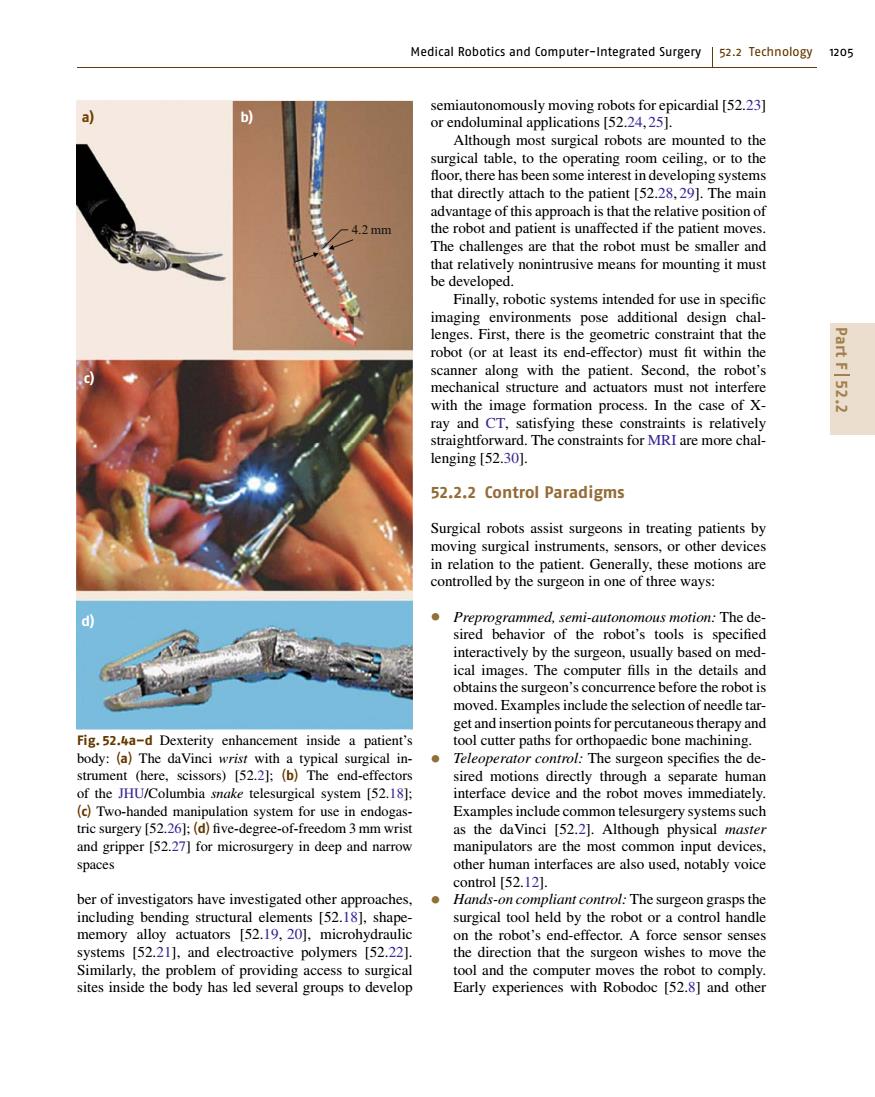
Medical Robotics and Computer-Integrated Surgery 52.2 Technology 1205 semiautonomously moving robots for epicardial [52.23] b or endoluminal applications [52.24,25]. Although most surgical robots are mounted to the surgical table,to the operating room ceiling,or to the floor,there has been some interest in developing systems that directly attach to the patient [52.28,29].The main advantage of this approach is that the relative position of 4.2mm the robot and patient is unaffected if the patient moves. The challenges are that the robot must be smaller and that relatively nonintrusive means for mounting it must be developed. Finally,robotic systems intended for use in specific imaging environments pose additional design chal- lenges.First,there is the geometric constraint that the robot (or at least its end-effector)must fit within the scanner along with the patient.Second,the robot's mechanical structure and actuators must not interfere Part F52 with the image formation process.In the case of X- ray and CT,satisfying these constraints is relatively straightforward.The constraints for MRI are more chal- lenging [52.30]. 52.2.2 Control Paradigms Surgical robots assist surgeons in treating patients by moving surgical instruments,sensors,or other devices in relation to the patient.Generally,these motions are controlled by the surgeon in one of three ways: d Preprogrammed,semi-autonomous motion:The de- sired behavior of the robot's tools is specified interactively by the surgeon,usually based on med- ical images.The computer fills in the details and obtains the surgeon's concurrence before the robot is moved.Examples include the selection of needle tar- get and insertion points for percutaneous therapy and Fig.52.4a-d Dexterity enhancement inside a patient's tool cutter paths for orthopaedic bone machining. body:(a)The daVinci wrist with a typical surgical in- Teleoperator control:The surgeon specifies the de- strument (here,scissors)[52.2]:(b)The end-effectors sired motions directly through a separate human of the JHU/Columbia snake telesurgical system [52.18]; interface device and the robot moves immediately. (c)Two-handed manipulation system for use in endogas- Examples include common telesurgery systems such tric surgery [52.26]:(d)five-degree-of-freedom 3 mm wrist as the daVinci [52.2].Although physical master and gripper [52.27]for microsurgery in deep and narrow manipulators are the most common input devices, spaces other human interfaces are also used,notably voice control [52.12]. ber of investigators have investigated other approaches,.Hands-on compliant control:The surgeon grasps the including bending structural elements [52.18],shape- surgical tool held by the robot or a control handle memory alloy actuators [52.19,20],microhydraulic on the robot's end-effector.A force sensor senses systems [52.21],and electroactive polymers [52.22]. the direction that the surgeon wishes to move the Similarly,the problem of providing access to surgical tool and the computer moves the robot to comply sites inside the body has led several groups to develop Early experiences with Robodoc [52.8]and otherMedical Robotics and Computer-Integrated Surgery 52.2 Technology 1205 4.2 mm b) c) d) a) Fig. 52.4a–d Dexterity enhancement inside a patient’s body: (a) The daVinci wrist with a typical surgical instrument (here, scissors) [52.2]; (b) The end-effectors of the JHU/Columbia snake telesurgical system [52.18]; (c) Two-handed manipulation system for use in endogastric surgery [52.26]; (d) five-degree-of-freedom 3 mm wrist and gripper [52.27] for microsurgery in deep and narrow spaces ber of investigators have investigated other approaches, including bending structural elements [52.18], shapememory alloy actuators [52.19, 20], microhydraulic systems [52.21], and electroactive polymers [52.22]. Similarly, the problem of providing access to surgical sites inside the body has led several groups to develop semiautonomously moving robots for epicardial [52.23] or endoluminal applications [52.24, 25]. Although most surgical robots are mounted to the surgical table, to the operating room ceiling, or to the floor, there has been some interest in developing systems that directly attach to the patient [52.28, 29]. The main advantage of this approach is that the relative position of the robot and patient is unaffected if the patient moves. The challenges are that the robot must be smaller and that relatively nonintrusive means for mounting it must be developed. Finally, robotic systems intended for use in specific imaging environments pose additional design challenges. First, there is the geometric constraint that the robot (or at least its end-effector) must fit within the scanner along with the patient. Second, the robot’s mechanical structure and actuators must not interfere with the image formation process. In the case of Xray and CT, satisfying these constraints is relatively straightforward. The constraints for MRI are more challenging [52.30]. 52.2.2 Control Paradigms Surgical robots assist surgeons in treating patients by moving surgical instruments, sensors, or other devices in relation to the patient. Generally, these motions are controlled by the surgeon in one of three ways: • Preprogrammed, semi-autonomous motion: The desired behavior of the robot’s tools is specified interactively by the surgeon, usually based on medical images. The computer fills in the details and obtains the surgeon’s concurrence before the robot is moved. Examples include the selection of needle target and insertion points for percutaneous therapy and tool cutter paths for orthopaedic bone machining. • Teleoperator control: The surgeon specifies the desired motions directly through a separate human interface device and the robot moves immediately. Examples include common telesurgery systems such as the daVinci [52.2]. Although physical master manipulators are the most common input devices, other human interfaces are also used, notably voice control [52.12]. • Hands-on compliant control: The surgeon grasps the surgical tool held by the robot or a control handle on the robot’s end-effector. A force sensor senses the direction that the surgeon wishes to move the tool and the computer moves the robot to comply. Early experiences with Robodoc [52.8] and other Part F 52.2