正在加载图片...
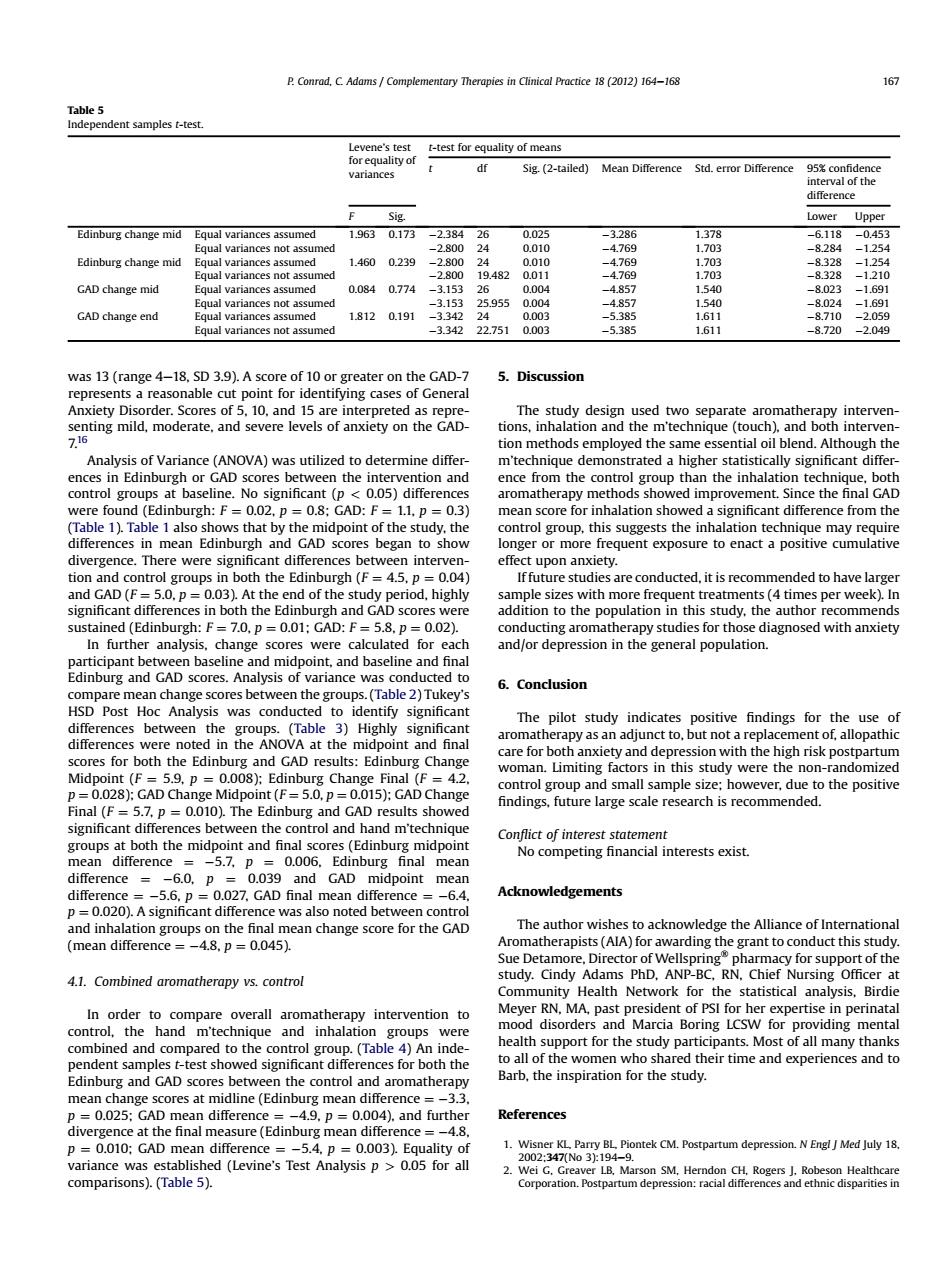
P.Conrad,C.Adams Complementary Therapies in Clinical Practice 18(2012)164-168 167 Table 5 Independent samples t-test Levene's test t-test for equality of means for equality of df variances Sig.(2-tailed)Mean Difference Std.error Difference 95%confidence interval of the ditterence Sig. Lower Upper Edinburg change mid Equal variances assumed 19630.173-2.38426 0025 -3.286 1.378 -6.118-0.453 Equal variances not assumed -2.800 24 0.010 -4.769 1.703 -8.284 -1.254 Edinburg change mid Equal variances assumed 1.4600.239 -2.800 24 0.010 -4.769 1.703 -8.328 -1.254 Equal variances not assumed -2800 19.4820011 -4769 1.703 -8.328 -1210 GAD change mid Equal variances assumed 0.084 0.774 -3.153 26 0.004 -4.857 1.540 -8.023 -1691 Equal variances not assumed -3.153 25.955 0004 -4857 1.540 -8024 -1691 GAD change end Equal variances assumed 1.8120.191 -3.342 24 0.003 -5.385 1.611 -8.710 -2.059 Equal variances not assumed -3.342 22.7510.003 -5.385 1.611 -8.720 -2.049 was 13 (range 4-18,SD 3.9).A score of 10 or greater on the GAD-7 5.Discussion represents a reasonable cut point for identifying cases of General Anxiety Disorder.Scores of 5.10,and 15 are interpreted as repre- The study design used two separate aromatherapy interven- senting mild,moderate,and severe levels of anxiety on the GAD- tions,inhalation and the m'technique(touch),and both interven- 7.16 tion methods employed the same essential oil blend.Although the Analysis of Variance(ANOVA)was utilized to determine differ- m'technique demonstrated a higher statistically significant differ- ences in Edinburgh or GAD scores between the intervention and ence from the control group than the inhalation technique,both control groups at baseline.No significant (p<0.05)differences aromatherapy methods showed improvement.Since the final GAD were found (Edinburgh:F=0.02,p=0.8;GAD:F=1.1,p =0.3) mean score for inhalation showed a significant difference from the (Table 1).Table 1 also shows that by the midpoint of the study,the control group,this suggests the inhalation technique may require differences in mean Edinburgh and GAD scores began to show longer or more frequent exposure to enact a positive cumulative divergence.There were significant differences between interven- effect upon anxiety. tion and control groups in both the Edinburgh (F=4.5,p =0.04) If future studies are conducted,it is recommended to have larger and GAD(F=5.0.p=0.03).At the end of the study period,highly sample sizes with more frequent treatments (4 times per week).In significant differences in both the Edinburgh and GAD scores were addition to the population in this study,the author recommends sustained (Edinburgh:F=7.0,p=0.01;GAD:F=5.8,p=0.02). conducting aromatherapy studies for those diagnosed with anxiety In further analysis,change scores were calculated for each and/or depression in the general population. participant between baseline and midpoint,and baseline and final Edinburg and GAD scores.Analysis of variance was conducted to 6.Conclusion compare mean change scores between the groups.(Table 2)Tukey's HSD Post Hoc Analysis was conducted to identify significant The pilot study indicates positive findings for the use of differences between the groups.(Table 3)Highly significant aromatherapy as an adjunct to,but not a replacement of,allopathic differences were noted in the ANOVA at the midpoint and final care for both anxiety and depression with the high risk postpartum scores for both the Edinburg and GAD results:Edinburg Change woman.Limiting factors in this study were the non-randomized Midpoint (F=5.9,p=0.008);Edinburg Change Final (F=4.2 control group and small sample size:however,due to the positive p=0.028);GAD Change Midpoint(F=5.0,p=0.015);GAD Change findings,future large scale research is recommended. Final (F=5.7,p=0.010).The Edinburg and GAD results showed significant differences between the control and hand m'technique Conflict of interest statement groups at both the midpoint and final scores(Edinburg midpoint No competing financial interests exist. mean difference =-5.7,p 0.006,Edinburg final mean difference =-6.0,p =0.039 and GAD midpoint mean difference =-5.6,p =0.027,GAD final mean difference =-6.4. Acknowledgements p=0.020).A significant difference was also noted between control and inhalation groups on the final mean change score for the GAD The author wishes to acknowledge the Alliance of International (mean difference =-4.8,p =0.045). Aromatherapists(AlA)for awarding the grant to conduct this study. Sue Detamore,Director of Wellspring pharmacy for support of the 4.1.Combined aromatherapy vs.control study.Cindy Adams PhD,ANP-BC,RN,Chief Nursing Officer at Community Health Network for the statistical analysis,Birdie In order to compare overall aromatherapy intervention to Meyer RN,MA,past president of PSI for her expertise in perinatal control,the hand m'technique and inhalation groups were mood disorders and Marcia Boring LCSW for providing mental combined and compared to the control group.(Table 4)An inde- health support for the study participants.Most of all many thanks pendent samples t-test showed significant differences for both the to all of the women who shared their time and experiences and to Edinburg and GAD scores between the control and aromatherapy Barb,the inspiration for the study. mean change scores at midline(Edinburg mean difference =-3.3. p=0.025;GAD mean difference =-4.9,p 0.004).and further References divergence at the final measure (Edinburg mean difference =-4.8, p=0.010;GAD mean difference =-5.4,p =0.003).Equality of 1.Wisner KL Parry BL Piontek CM.Postpartum depression.N Engl J Med July 18. variance was established (Levine's Test Analysis p>0.05 for all 2002:347No3194-9. 2.Wei G.Greaver LB.Marson SM,Herndon CH,Rogers J.Robeson Healthcare comparisons).(Table 5). Corporation.Postpartum depression:racial differences and ethnic disparities inwas 13 (range 4e18, SD 3.9). A score of 10 or greater on the GAD-7 represents a reasonable cut point for identifying cases of General Anxiety Disorder. Scores of 5, 10, and 15 are interpreted as representing mild, moderate, and severe levels of anxiety on the GAD- 7.16 Analysis of Variance (ANOVA) was utilized to determine differences in Edinburgh or GAD scores between the intervention and control groups at baseline. No significant (p < 0.05) differences were found (Edinburgh: F ¼ 0.02, p ¼ 0.8; GAD: F ¼ 1.1, p ¼ 0.3) (Table 1). Table 1 also shows that by the midpoint of the study, the differences in mean Edinburgh and GAD scores began to show divergence. There were significant differences between intervention and control groups in both the Edinburgh (F ¼ 4.5, p ¼ 0.04) and GAD (F ¼ 5.0, p ¼ 0.03). At the end of the study period, highly significant differences in both the Edinburgh and GAD scores were sustained (Edinburgh: F ¼ 7.0, p ¼ 0.01; GAD: F ¼ 5.8, p ¼ 0.02). In further analysis, change scores were calculated for each participant between baseline and midpoint, and baseline and final Edinburg and GAD scores. Analysis of variance was conducted to compare mean change scores between the groups. (Table 2) Tukey’s HSD Post Hoc Analysis was conducted to identify significant differences between the groups. (Table 3) Highly significant differences were noted in the ANOVA at the midpoint and final scores for both the Edinburg and GAD results: Edinburg Change Midpoint (F ¼ 5.9, p ¼ 0.008); Edinburg Change Final (F ¼ 4.2, p ¼ 0.028); GAD Change Midpoint (F ¼ 5.0, p ¼ 0.015); GAD Change Final (F ¼ 5.7, p ¼ 0.010). The Edinburg and GAD results showed significant differences between the control and hand m’technique groups at both the midpoint and final scores (Edinburg midpoint mean difference ¼ 5.7, p ¼ 0.006, Edinburg final mean difference ¼ 6.0, p ¼ 0.039 and GAD midpoint mean difference ¼ 5.6, p ¼ 0.027, GAD final mean difference ¼ 6.4, p ¼ 0.020). A significant difference was also noted between control and inhalation groups on the final mean change score for the GAD (mean difference ¼ 4.8, p ¼ 0.045). 4.1. Combined aromatherapy vs. control In order to compare overall aromatherapy intervention to control, the hand m’technique and inhalation groups were combined and compared to the control group. (Table 4) An independent samples t-test showed significant differences for both the Edinburg and GAD scores between the control and aromatherapy mean change scores at midline (Edinburg mean difference ¼ 3.3, p ¼ 0.025; GAD mean difference ¼ 4.9, p ¼ 0.004), and further divergence at the final measure (Edinburg mean difference ¼ 4.8, p ¼ 0.010; GAD mean difference ¼ 5.4, p ¼ 0.003). Equality of variance was established (Levine’s Test Analysis p > 0.05 for all comparisons). (Table 5). 5. Discussion The study design used two separate aromatherapy interventions, inhalation and the m’technique (touch), and both intervention methods employed the same essential oil blend. Although the m’technique demonstrated a higher statistically significant difference from the control group than the inhalation technique, both aromatherapy methods showed improvement. Since the final GAD mean score for inhalation showed a significant difference from the control group, this suggests the inhalation technique may require longer or more frequent exposure to enact a positive cumulative effect upon anxiety. If future studies are conducted, it is recommended to have larger sample sizes with more frequent treatments (4 times per week). In addition to the population in this study, the author recommends conducting aromatherapy studies for those diagnosed with anxiety and/or depression in the general population. 6. Conclusion The pilot study indicates positive findings for the use of aromatherapy as an adjunct to, but not a replacement of, allopathic care for both anxiety and depression with the high risk postpartum woman. Limiting factors in this study were the non-randomized control group and small sample size; however, due to the positive findings, future large scale research is recommended. Conflict of interest statement No competing financial interests exist. Acknowledgements The author wishes to acknowledge the Alliance of International Aromatherapists (AIA) for awarding the grant to conduct this study. Sue Detamore, Director of Wellspring pharmacy for support of the study. Cindy Adams PhD, ANP-BC, RN, Chief Nursing Officer at Community Health Network for the statistical analysis, Birdie Meyer RN, MA, past president of PSI for her expertise in perinatal mood disorders and Marcia Boring LCSW for providing mental health support for the study participants. Most of all many thanks to all of the women who shared their time and experiences and to Barb, the inspiration for the study. References 1. Wisner KL, Parry BL, Piontek CM. Postpartum depression. N Engl J Med July 18, 2002;347(No 3):194e9. 2. Wei G, Greaver LB, Marson SM, Herndon CH, Rogers J, Robeson Healthcare Corporation. Postpartum depression: racial differences and ethnic disparities in Table 5 Independent samples t-test. Levene’s test for equality of variances t-test for equality of means t df Sig. (2-tailed) Mean Difference Std. error Difference 95% confidence interval of the difference F Sig. Lower Upper Edinburg change mid Equal variances assumed 1.963 0.173 2.384 26 0.025 3.286 1.378 6.118 0.453 Equal variances not assumed 2.800 24 0.010 4.769 1.703 8.284 1.254 Edinburg change mid Equal variances assumed 1.460 0.239 2.800 24 0.010 4.769 1.703 8.328 1.254 Equal variances not assumed 2.800 19.482 0.011 4.769 1.703 8.328 1.210 GAD change mid Equal variances assumed 0.084 0.774 3.153 26 0.004 4.857 1.540 8.023 1.691 Equal variances not assumed 3.153 25.955 0.004 4.857 1.540 8.024 1.691 GAD change end Equal variances assumed 1.812 0.191 3.342 24 0.003 5.385 1.611 8.710 2.059 Equal variances not assumed 3.342 22.751 0.003 5.385 1.611 8.720 2.049 P. Conrad, C. Adams / Complementary Therapies in Clinical Practice 18 (2012) 164e168 167������������������������������������������