正在加载图片...
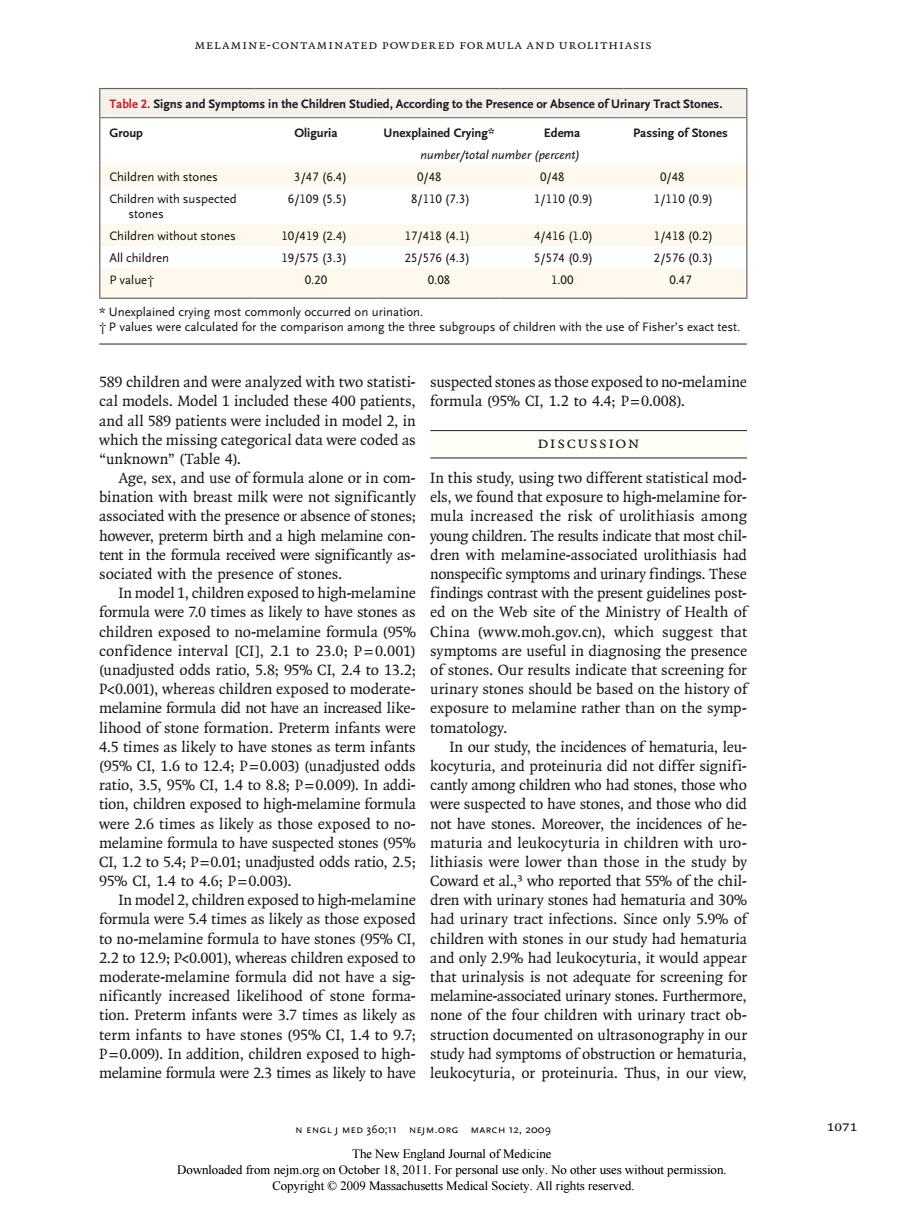
MELAMINE-CONTAMINATED POWDERED FORMULA AND UROLITHIASIS Table2.Signs and Symptoms in the Children Studied,According to the Presenceor Absence of Urinary Tract Stones Group Oliguria Unexplained Crying Edema Passing of Stones number/total number (percent) Children with stones 3/4716.4 0/48 0/48 0/48 Children with suspected 61095.5引 8/1107.3) 11100.9) 1/1100.9y stones Children without stones 10/419(2.4 17/418(4.1 4/416(1.0 1/418(0.2 All children 19/5753.3) 25/576(4.3) 5/5740.9) 2/576(0.3) P valuet 0.20 0.08 1.00 0.47 only occurred on urination caate or the comprithe three subous of children with the use of Fisheat test 589 children and were analyzed with two statisti- suspected stones as those exposed to no-melamine cal models.Model 1 included these 400 patients, formula95%CL,12to4.4:P=0.008). and all 589 patients were included in model 2,ir which the mis data were coded as DIscUSSIOn e In this study,using two differen tical mod. ast milk y els we found that to high-melamine for associated with the presence or absence of stones:mula increased the risk of urolithiasis among however,preterm birth and a high melamine con-young children.The results indicate that most chil tent in the formula received were significantly as- dren with melamine-associated urolithiasis hac sociated witht he presence of stor nonspecific symptoms and urinary find dings.Ines hild were 0 In m en ex to hig h-melamin ast wit likel 1a (058 confidence interval [CI.2.1 to 23.0:P=0.001) ntoms are useful in diagnosing th (unadjusted odds ratio,5.8%Cl.2.4 to 13.2:of stones.Our results indicate that screening for P<0.001),whereas children exposed to moderate- urinary stones should be based on the history of melamine formula did not have an increased like exposure to melamine rather than on the symp lihood of stone formation.Preterm inant tomatology. 45C16o224 D-0003 dy,the incide of hem atio,35,95%CL,1.4to8.8p= o0o In addi tion children exposed to high-melamine formula were suspected to have stones and those who did were 2.6 times as likely as those exposed to no- not have stones.Moreover the incidences of he melamine formula to have suspected stones (95% maturia and leukocyturia in children with uro Cl,1.2 to5.4;P0.01;unadjusted odds ratio,.5; lithiasis were lo wer than t se in the study 05 odel ,who report at55% ren ex vith had u tract nges ns.Sima d c only 5 9%of tones (05 children with stones in our study had hematuria 22 to 12 9:P<o001)whereas children exposed to and only 2 9%had leukocyturia it would appea moderate-melamine formula did not have a sig-that urinalysis is not adequate for screening for nificantly increased likelihood of stone tion. reterm inra nts we 5. none of th ren th urinary t ve st s(95%CL,1 ocumente n0 graphy in ou nelamine formula N ENGLJ MED 360,11 NEJM.ORG MARCH 12,2009 1071 The New Englar nd Journal of Medicine thout permission Melamine-Contaminated Powdered Formula and Urolithiasis n engl j med 360;11 nejm.org march 12, 2009 1071 589 children and were analyzed with two statistical models. Model 1 included these 400 patients, and all 589 patients were included in model 2, in which the missing categorical data were coded as “unknown” (Table 4). Age, sex, and use of formula alone or in combination with breast milk were not significantly associated with the presence or absence of stones; however, preterm birth and a high melamine content in the formula received were significantly associated with the presence of stones. In model 1, children exposed to high-melamine formula were 7.0 times as likely to have stones as children exposed to no-melamine formula (95% confidence interval [CI], 2.1 to 23.0; P=0.001) (unadjusted odds ratio, 5.8; 95% CI, 2.4 to 13.2; P<0.001), whereas children exposed to moderatemelamine formula did not have an increased likelihood of stone formation. Preterm infants were 4.5 times as likely to have stones as term infants (95% CI, 1.6 to 12.4; P=0.003) (unadjusted odds ratio, 3.5, 95% CI, 1.4 to 8.8; P=0.009). In addition, children exposed to high-melamine formula were 2.6 times as likely as those exposed to nomelamine formula to have suspected stones (95% CI, 1.2 to 5.4; P=0.01; unadjusted odds ratio, 2.5; 95% CI, 1.4 to 4.6; P=0.003). In model 2, children exposed to high-melamine formula were 5.4 times as likely as those exposed to no-melamine formula to have stones (95% CI, 2.2 to 12.9; P<0.001), whereas children exposed to moderate-melamine formula did not have a significantly increased likelihood of stone formation. Preterm infants were 3.7 times as likely as term infants to have stones (95% CI, 1.4 to 9.7; P=0.009). In addition, children exposed to highmelamine formula were 2.3 times as likely to have suspected stones as those exposed to no-melamine formula (95% CI, 1.2 to 4.4; P=0.008). Discussion In this study, using two different statistical models, we found that exposure to high-melamine formula increased the risk of urolithiasis among young children. The results indicate that most children with melamine-associated urolithiasis had nonspecific symptoms and urinary findings. These findings contrast with the present guidelines posted on the Web site of the Ministry of Health of China (www.moh.gov.cn), which suggest that symptoms are useful in diagnosing the presence of stones. Our results indicate that screening for urinary stones should be based on the history of exposure to melamine rather than on the symptomatology. In our study, the incidences of hematuria, leukocyturia, and proteinuria did not differ significantly among children who had stones, those who were suspected to have stones, and those who did not have stones. Moreover, the incidences of hematuria and leukocyturia in children with urolithiasis were lower than those in the study by Coward et al.,3 who reported that 55% of the children with urinary stones had hematuria and 30% had urinary tract infections. Since only 5.9% of children with stones in our study had hematuria and only 2.9% had leukocyturia, it would appear that urinalysis is not adequate for screening for melamine-associated urinary stones. Furthermore, none of the four children with urinary tract obstruction documented on ultrasonography in our study had symptoms of obstruction or hematuria, leukocyturia, or proteinuria. Thus, in our view, Table 2. Signs and Symptoms in the Children Studied, According to the Presence or Absence of Urinary Tract Stones. Group Oliguria Unexplained Crying* Edema Passing of Stones number/total number (percent) Children with stones 3/47 (6.4) 0/48 0/48 0/48 Children with suspected stones 6/109 (5.5) 8/110 (7.3) 1/110 (0.9) 1/110 (0.9) Children without stones 10/419 (2.4) 17/418 (4.1) 4/416 (1.0) 1/418 (0.2) All children 19/575 (3.3) 25/576 (4.3) 5/574 (0.9) 2/576 (0.3) P value† 0.20 0.08 1.00 0.47 * Unexplained crying most commonly occurred on urination. † P values were calculated for the comparison among the three subgroups of children with the use of Fisher’s exact test. The New England Journal of Medicine Downloaded from nejm.org on October 18, 2011. For personal use only. No other uses without permission. Copyright © 2009 Massachusetts Medical Society. All rights reserved