正在加载图片...
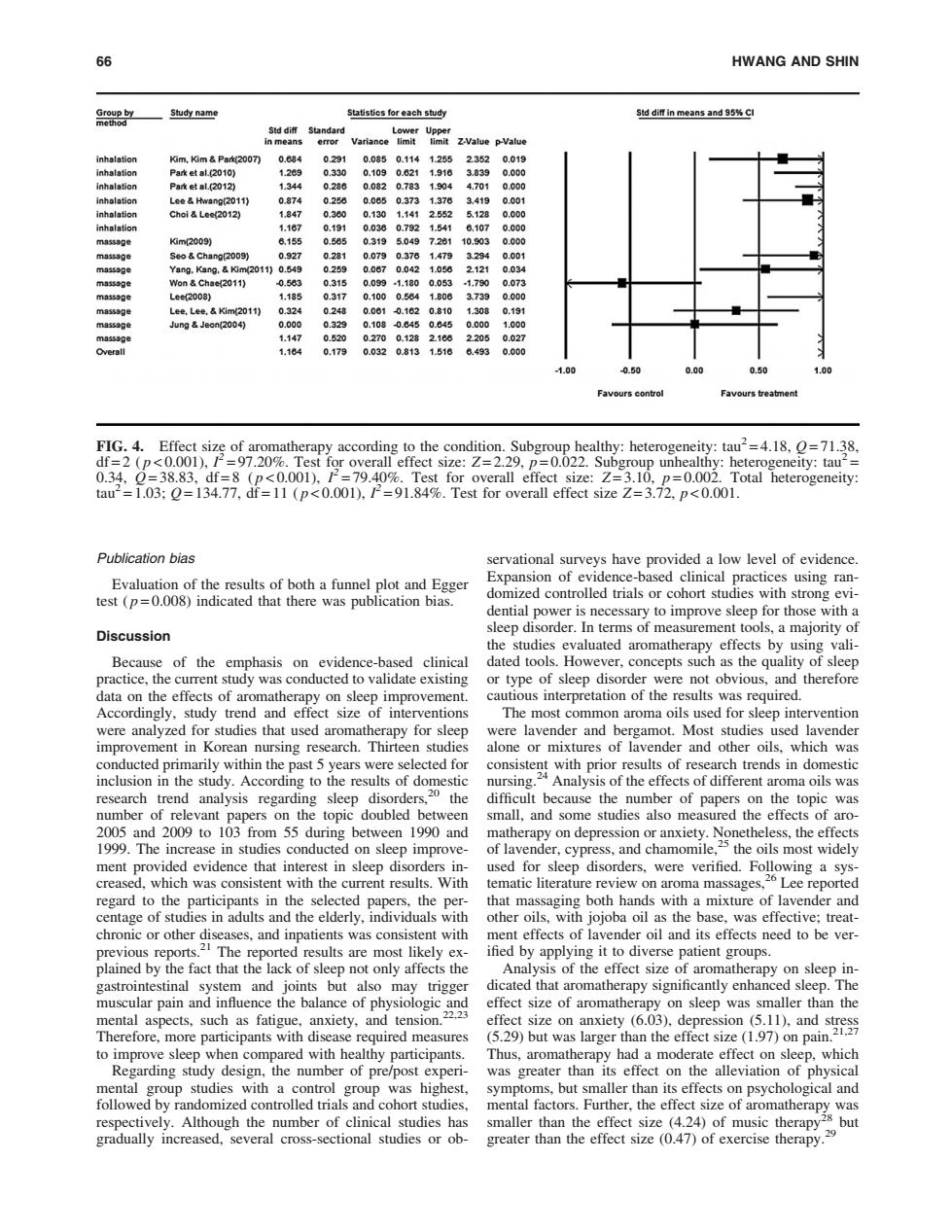
66 HWANG AND SHIN Group by Study name Statistics for each study Std diff in means and 95%CI method Std diff Standard in means Variance inhalation 灯m,灯m&Pa200刀 0.084 0.291 0.0850.1141.255 2.352 0.019 inhalation Park et al.(2010) 1.289 0.330 0.1090.821 1.916 3.839 0.000 inhalation P8keta12012列 1344 0.286 0.0820.7831.904 4.701 0.000 inhalation Lee Hwang(2011) 0.874 0.258 0.08503731378 3.419 0.001 inhalation Choi Lee(2012) 1.847 0.380 0.130 1.141 2.552 5128 0.000 inhalation 1.187 0.191 0.0380.7921.541 8.107 0.000 massage 灯m2009) 6,155 0.585 031950497281 10.903 0.000 massage Seo Chang(2009) 0.927 0.281 0.0790.378 1.479 3294 0.001 massage Yang.Kang.Kim(2011)0.549 0.259 0.0870.042 1.058 2.121 0.034 mn553a色 Won Chae(2011) -0.583 0.315 0.0991.1800.053 -1.790 0.073 massage Lee2008) 1.,185 0.317 0.100 0.684 1.806 3739 0.000 massage Lee.Lee.Kim(2011) 0.324 0.248 0.081 -0.162 0.810 1.308 0.191 massage Jung Jeon(2004) 0.000 0.329 0.108-0.8450.845 0.000 1.000 m35539e 1.147 0.520 02700.128 2188 2205 0.027 1.164 0.179 0.0320.8131.516 6.493 0.000 1.00 0.50 .00 Favours controt Favours treatment FIG.4.Effect size of aromatherapy according to the condition.Subgroup healthy:heterogeneity:tau2=4.18,O=71.38. df=2 (p<0.001),/=97.20%.Test for overall effect size:Z=2.29,p=0.022.Subgroup unhealthy:heterogeneity:tau2= 0.34,0=38.83,df=8 (p<0.001),12=79.40%.Test for overall effect size:Z=3.10,p=0.002.Total heterogeneity: tau2=1.03;O=134.77,df=11 (p<0.001),P=91.84%.Test for overall effect size Z=3.72,p<0.001. Publication bias servational surveys have provided a low level of evidence. Evaluation of the results of both a funnel plot and Egger Expansion of evidence-based clinical practices using ran- test (p=0.008)indicated that there was publication bias. domized controlled trials or cohort studies with strong evi- dential power is necessary to improve sleep for those with a Discussion sleep disorder.In terms of measurement tools,a majority of the studies evaluated aromatherapy effects by using vali- Because of the emphasis on evidence-based clinical dated tools.However.concepts such as the quality of sleep practice,the current study was conducted to validate existing or type of sleep disorder were not obvious,and therefore data on the effects of aromatherapy on sleep improvement. cautious interpretation of the results was required Accordingly,study trend and effect size of interventions The most common aroma oils used for sleep intervention were analyzed for studies that used aromatherapy for sleep were lavender and bergamot.Most studies used lavender improvement in Korean nursing research.Thirteen studies alone or mixtures of lavender and other oils,which was conducted primarily within the past 5 years were selected for consistent with prior results of research trends in domestic inclusion in the study.According to the results of domestic nursing. .24 Analysis of the effects of different aroma oils was research trend analysis regarding sleep disorders,20 the difficult because the number of papers on the topic was number of relevant papers on the topic doubled between small,and some studies also measured the effects of aro- 2005 and 2009 to 103 from 55 during between 1990 and matherapy on depression or anxiety.Nonetheless,the effects 1999.The increase in studies conducted on sleep improve- of lavender,cypress,and chamomile,the oils most widely ment provided evidence that interest in sleep disorders in- used for sleep disorders,were verified.Following a sys- creased,which was consistent with the current results.With tematic literature review on aroma massages,26 Lee reported regard to the participants in the selected papers,the per- that massaging both hands with a mixture of lavender and centage of studies in adults and the elderly,individuals with other oils,with jojoba oil as the base,was effective;treat- chronic or other diseases,and inpatients was consistent with ment effects of lavender oil and its effects need to be ver- previous reports.2 The reported results are most likely ex- ified by applying it to diverse patient groups. plained by the fact that the lack of sleep not only affects the Analysis of the effect size of aromatherapy on sleep in- gastrointestinal system and joints but also may trigger dicated that aromatherapy significantly enhanced sleep.The muscular pain and influence the balance of physiologic and effect size of aromatherapy on sleep was smaller than the mental aspects,such as fatigue,anxiety,and tension.22.23 effect size on anxiety (6.03).depression(5.11),and stress Therefore,more participants with disease required measures (5.29)but was larger than the effect size(1.97)on pain.21.27 to improve sleep when compared with healthy participants. Thus,aromatherapy had a moderate effect on sleep,which Regarding study design,the number of pre/post experi- was greater than its effect on the alleviation of physical mental group studies with a control group was highest, symptoms,but smaller than its effects on psychological and followed by randomized controlled trials and cohort studies, mental factors.Further,the effect size of aromatherapy was respectively.Although the number of clinical studies has smaller than the effect size (4.24)of music therapy 28 but gradually increased,several cross-sectional studies or ob-greater than the effect size (0.47)of exercise therapy. 9Publication bias Evaluation of the results of both a funnel plot and Egger test ( p = 0.008) indicated that there was publication bias. Discussion Because of the emphasis on evidence-based clinical practice, the current study was conducted to validate existing data on the effects of aromatherapy on sleep improvement. Accordingly, study trend and effect size of interventions were analyzed for studies that used aromatherapy for sleep improvement in Korean nursing research. Thirteen studies conducted primarily within the past 5 years were selected for inclusion in the study. According to the results of domestic research trend analysis regarding sleep disorders,20 the number of relevant papers on the topic doubled between 2005 and 2009 to 103 from 55 during between 1990 and 1999. The increase in studies conducted on sleep improvement provided evidence that interest in sleep disorders increased, which was consistent with the current results. With regard to the participants in the selected papers, the percentage of studies in adults and the elderly, individuals with chronic or other diseases, and inpatients was consistent with previous reports.21 The reported results are most likely explained by the fact that the lack of sleep not only affects the gastrointestinal system and joints but also may trigger muscular pain and influence the balance of physiologic and mental aspects, such as fatigue, anxiety, and tension.22,23 Therefore, more participants with disease required measures to improve sleep when compared with healthy participants. Regarding study design, the number of pre/post experimental group studies with a control group was highest, followed by randomized controlled trials and cohort studies, respectively. Although the number of clinical studies has gradually increased, several cross-sectional studies or observational surveys have provided a low level of evidence. Expansion of evidence-based clinical practices using randomized controlled trials or cohort studies with strong evidential power is necessary to improve sleep for those with a sleep disorder. In terms of measurement tools, a majority of the studies evaluated aromatherapy effects by using validated tools. However, concepts such as the quality of sleep or type of sleep disorder were not obvious, and therefore cautious interpretation of the results was required. The most common aroma oils used for sleep intervention were lavender and bergamot. Most studies used lavender alone or mixtures of lavender and other oils, which was consistent with prior results of research trends in domestic nursing.24 Analysis of the effects of different aroma oils was difficult because the number of papers on the topic was small, and some studies also measured the effects of aromatherapy on depression or anxiety. Nonetheless, the effects of lavender, cypress, and chamomile,25 the oils most widely used for sleep disorders, were verified. Following a systematic literature review on aroma massages,26 Lee reported that massaging both hands with a mixture of lavender and other oils, with jojoba oil as the base, was effective; treatment effects of lavender oil and its effects need to be verified by applying it to diverse patient groups. Analysis of the effect size of aromatherapy on sleep indicated that aromatherapy significantly enhanced sleep. The effect size of aromatherapy on sleep was smaller than the effect size on anxiety (6.03), depression (5.11), and stress (5.29) but was larger than the effect size (1.97) on pain.21,27 Thus, aromatherapy had a moderate effect on sleep, which was greater than its effect on the alleviation of physical symptoms, but smaller than its effects on psychological and mental factors. Further, the effect size of aromatherapy was smaller than the effect size (4.24) of music therapy28 but greater than the effect size (0.47) of exercise therapy.29 FIG. 4. Effect size of aromatherapy according to the condition. Subgroup healthy: heterogeneity: tau2 = 4.18, Q = 71.38, df = 2 ( p < 0.001), I 2 = 97.20%. Test for overall effect size: Z = 2.29, p = 0.022. Subgroup unhealthy: heterogeneity: tau2 = 0.34, Q = 38.83, df = 8 ( p < 0.001), I 2 = 79.40%. Test for overall effect size: Z = 3.10, p = 0.002. Total heterogeneity: tau2 = 1.03; Q = 134.77, df = 11 ( p < 0.001), I 2 = 91.84%. Test for overall effect size Z = 3.72, p < 0.001. 66 HWANG AND SHIN