正在加载图片...
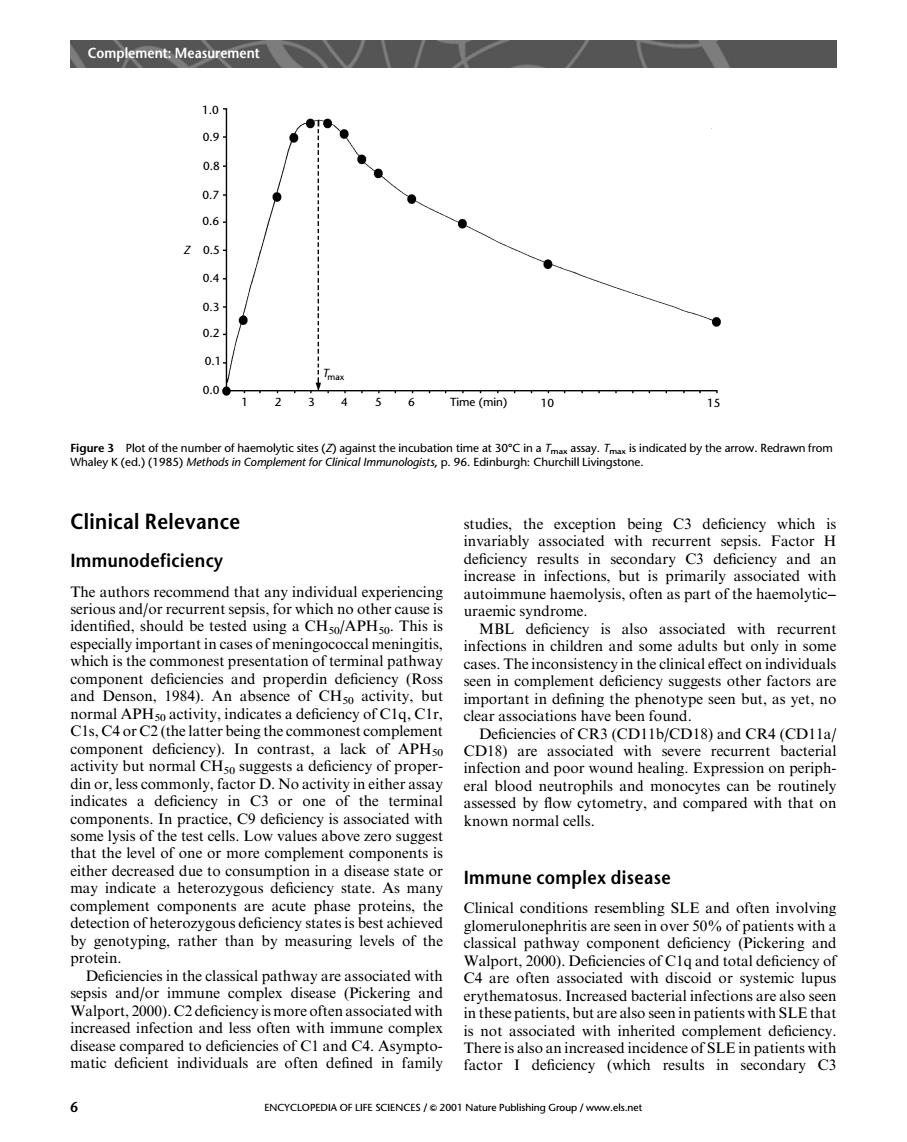
Complement:Measurement 1.0 0.9 0.8 0.6 z05 04 0.1 0.0 123456Tme(mn10 15 Clinical Relevance Immunodeficiency t or which no nng autoimmune haemolysis,often as part of the haemolytic- This is is also ass with recurren hic pccially important in cases of meningococcal meningitis. ommonest presentation of terminal pathway ases The inconsiste ncy in the clinical effect on individuals seen in complement deficiency suggests other factors are LAPH mportant in defining the phenotype seen but,as yet,no CIs C4or C the latter beins the commonest complement CD18)and CR4(CDIla CD18)are associated with severe recurrent bacterial one of the cidgponer infection and poor wound healing.Expression on periph- in C3 cr a components.In practice,C9 deficiency is associated with wn nor some lysis of the test cells.Low values above zero suggest the level of one or more complement compone nts state As mapy Immune complex disease complement components are acute phase proteins,the Clinical conditions resembling SLE and often involving detection of heterozygous deficiency states is best achieved glomerulonephritis are seen in over 50%of pa tients with by genotyping.rather than by measuring levels of the ssical pathway component deficiency (Pickering and Deficiencies in the classical nath ciated with ncies of Clq and total deficiency of are often ass in these patients,but arealso seen n patients with SLE that increased infection and une complex is not associated with inherited complement deficiency iiec2arnndasaeonc ciency (whic 6 ENCYCLOPEDIA OF LIFE SCIENCES/2001 Nature Publishing Group/www.els.net Clinical Relevance Immunodeficiency The authors recommend that any individual experiencing serious and/or recurrent sepsis, for which no other cause is identified, should be tested using a CH50/APH50. This is especially important in cases of meningococcal meningitis, which is the commonest presentation of terminal pathway component deficiencies and properdin deficiency (Ross and Denson, 1984). An absence of CH50 activity, but normal APH50 activity, indicates a deficiency of C1q, C1r, C1s, C4 or C2 (the latter being the commonest complement component deficiency). In contrast, a lack of APH50 activity but normal CH50 suggests a deficiency of properdin or, less commonly, factor D. No activity in either assay indicates a deficiency in C3 or one of the terminal components. In practice, C9 deficiency is associated with some lysis of the test cells. Low values above zero suggest that the level of one or more complement components is either decreased due to consumption in a disease state or may indicate a heterozygous deficiency state. As many complement components are acute phase proteins, the detection of heterozygous deficiency states is best achieved by genotyping, rather than by measuring levels of the protein. Deficiencies in the classical pathway are associated with sepsis and/or immune complex disease (Pickering and Walport, 2000). C2 deficiency is more often associated with increased infection and less often with immune complex disease compared to deficiencies of C1 and C4. Asymptomatic deficient individuals are often defined in family studies, the exception being C3 deficiency which is invariably associated with recurrent sepsis. Factor H deficiency results in secondary C3 deficiency and an increase in infections, but is primarily associated with autoimmune haemolysis, often as part of the haemolytic– uraemic syndrome. MBL deficiency is also associated with recurrent infections in children and some adults but only in some cases. The inconsistency in the clinical effect on individuals seen in complement deficiency suggests other factors are important in defining the phenotype seen but, as yet, no clear associations have been found. Deficiencies of CR3 (CD11b/CD18) and CR4 (CD11a/ CD18) are associated with severe recurrent bacterial infection and poor wound healing. Expression on peripheral blood neutrophils and monocytes can be routinely assessed by flow cytometry, and compared with that on known normal cells. Immune complex disease Clinical conditions resembling SLE and often involving glomerulonephritis are seen in over 50% of patients with a classical pathway component deficiency (Pickering and Walport, 2000). Deficiencies of C1q and total deficiency of C4 are often associated with discoid or systemic lupus erythematosus. Increased bacterial infections are also seen in these patients, but are also seen in patients with SLE that is not associated with inherited complement deficiency. There is also an increased incidence of SLE in patients with factor I deficiency (which results in secondary C3 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 1 2 3 4 5 6 Time (min) 10 15 T max Z Figure 3 Plot of the number of haemolytic sites (Z) against the incubation time at 308C in a Tmax assay. Tmax is indicated by the arrow. Redrawn from Whaley K (ed.) (1985) Methods in Complement for Clinical Immunologists, p. 96. Edinburgh: Churchill Livingstone. Complement: Measurement 6 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net