正在加载图片...
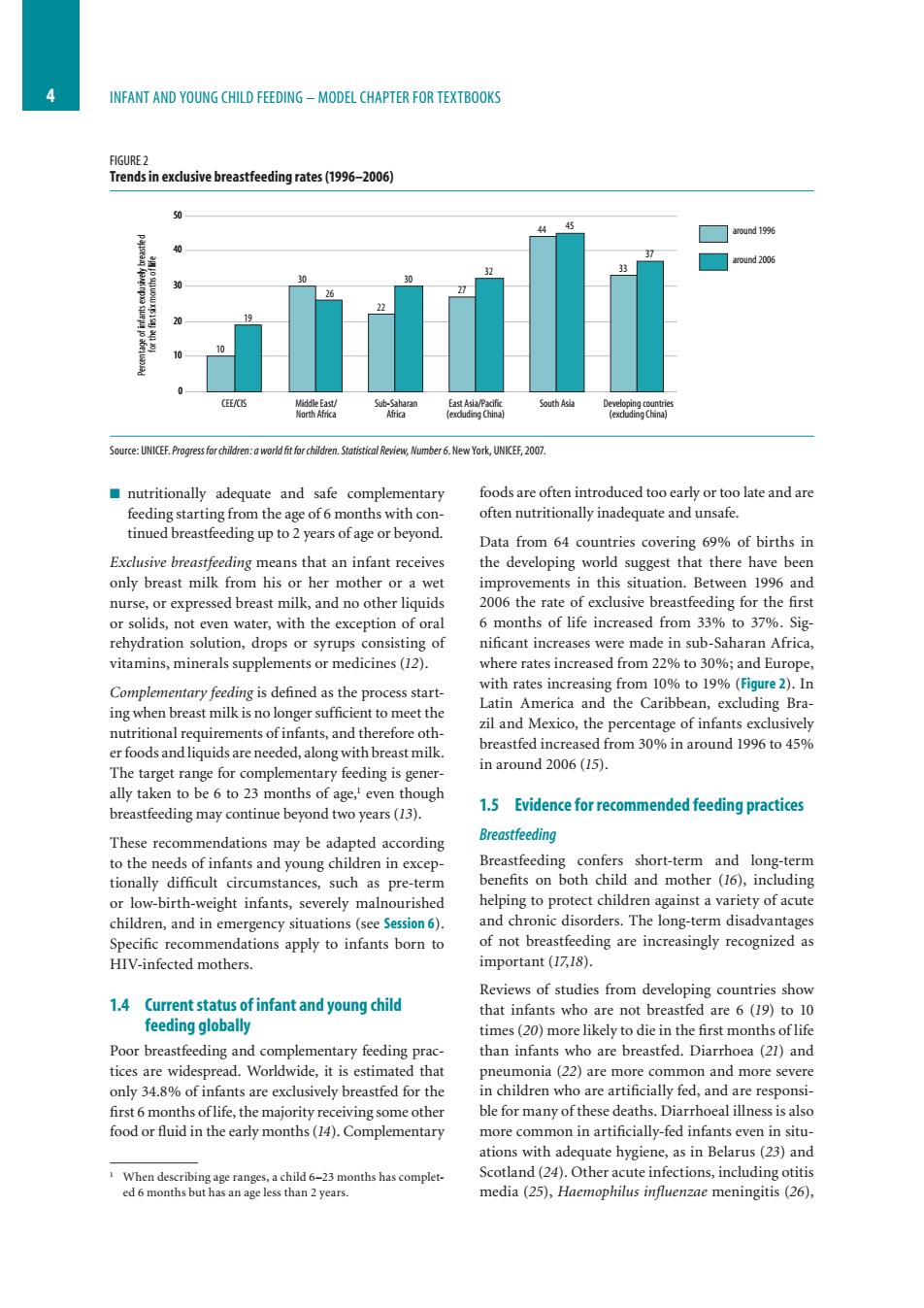
4 INFANT AND YOUNG CHILD FEEDING-MODEL CHAPTER FOR TEXTBOOKS FIGURE 2 Trends in exclusive breastfeeding rates(1996-2006) 50 20und1996 eround 2006 (EE还 Middle East/ Sub-Saharan East Asia/Pacific South Asi地 Developing countrie座 North Africa Africa (exduding China) (exduding Chinal Source:UNICEF.Progress for children:a world fit for children.Statistical Review,Number 6.New York,UNICEF,2007 nutritionally adequate and safe complementary foods are often introduced too early or too late and are feeding starting from the age of 6 months with con- often nutritionally inadequate and unsafe. tinued breastfeeding up to 2 years of age or beyond. Data from 64 countries covering 69%of births in Exclusive breastfeeding means that an infant receives the developing world suggest that there have been only breast milk from his or her mother or a wet improvements in this situation.Between 1996 and nurse,or expressed breast milk,and no other liquids 2006 the rate of exclusive breastfeeding for the first or solids,not even water,with the exception of oral 6 months of life increased from 33%to 37%.Sig- rehydration solution,drops or syrups consisting of nificant increases were made in sub-Saharan Africa, vitamins,minerals supplements or medicines(12). where rates increased from 22%to 30%;and Europe, Complementary feeding is defined as the process start- with rates increasing from 10%to 19%(Figure 2).In Latin America and the Caribbean,excluding Bra- ing when breast milk is no longer sufficient to meet the nutritional requirements of infants,and therefore oth- zil and Mexico,the percentage of infants exclusively er foods and liquids are needed,along with breast milk. breastfed increased from 30%in around 1996 to 45% The target range for complementary feeding is gener- in around 2006(15). ally taken to be 6 to 23 months of age,even though breastfeeding may continue beyond two years(13). 1.5 Evidence for recommended feeding practices These recommendations may be adapted according Breastfeeding to the needs of infants and young children in excep- Breastfeeding confers short-term and long-term tionally difficult circumstances,such as pre-term benefits on both child and mother (16),including or low-birth-weight infants,severely malnourished helping to protect children against a variety of acute children,and in emergency situations(see Session 6). and chronic disorders.The long-term disadvantages Specific recommendations apply to infants born to of not breastfeeding are increasingly recognized as HIV-infected mothers important(1718). Reviews of studies from developing countries show 1.4 Current status of infant and young child that infants who are not breastfed are 6(19)to 10 feeding globally times(20)more likely to die in the first months of life Poor breastfeeding and complementary feeding prac- than infants who are breastfed.Diarrhoea (21)and tices are widespread.Worldwide,it is estimated that pneumonia(22)are more common and more severe only 34.8%of infants are exclusively breastfed for the in children who are artificially fed,and are responsi- first 6 months oflife,the majority receiving some other ble for many of these deaths.Diarrhoeal illness is also food or fluid in the early months(14).Complementary more common in artificially-fed infants even in situ- ations with adequate hygiene,as in Belarus(23)and When describing age ranges,a child 6-23 months has complet- Scotland(24).Other acute infections,including otitis ed 6 months but has an age less than 2 years. media (25),Haemophilus influenzae meningitis (26),4 Infant and Young Child Feeding – Model Chapter for textbooks K nutritionally adequate and safe complementary feeding starting from the age of 6 months with continued breastfeeding up to 2 years of age or beyond. Exclusive breastfeeding means that an infant receives only breast milk from his or her mother or a wet nurse, or expressed breast milk, and no other liquids or solids, not even water, with the exception of oral rehydration solution, drops or syrups consisting of vitamins, minerals supplements or medicines (12). Complementary feeding is defined as the process starting when breast milk is no longer sufficient to meet the nutritional requirements of infants, and therefore other foods and liquids are needed, along with breast milk. The target range for complementary feeding is generally taken to be 6 to 23 months of age,1 even though breastfeeding may continue beyond two years (13). These recommendations may be adapted according to the needs of infants and young children in exceptionally difficult circumstances, such as pre-term or low-birth-weight infants, severely malnourished children, and in emergency situations (see Session 6). Specific recommendations apply to infants born to HIV-infected mothers. 1.4 Current status of infant and young child feeding globally Poor breastfeeding and complementary feeding practices are widespread. Worldwide, it is estimated that only 34.8% of infants are exclusively breastfed for the first 6 months of life, the majority receiving some other food or fluid in the early months (14). Complementary foods are often introduced too early or too late and are often nutritionally inadequate and unsafe. Data from 64 countries covering 69% of births in the developing world suggest that there have been improvements in this situation. Between 1996 and 2006 the rate of exclusive breastfeeding for the first 6 months of life increased from 33% to 37%. Significant increases were made in sub-Saharan Africa, where rates increased from 22% to 30%; and Europe, with rates increasing from 10% to 19% (Figure 2). In Latin America and the Caribbean, excluding Brazil and Mexico, the percentage of infants exclusively breastfed increased from 30% in around 1996 to 45% in around 2006 (15). 1.5 Evidence for recommended feeding practices Breastfeeding Breastfeeding confers short-term and long-term benefits on both child and mother (16), including helping to protect children against a variety of acute and chronic disorders. The long-term disadvantages of not breastfeeding are increasingly recognized as important (17,18). Reviews of studies from developing countries show that infants who are not breastfed are 6 (19) to 10 times (20) more likely to die in the first months of life than infants who are breastfed. Diarrhoea (21) and pneumonia (22) are more common and more severe in children who are artificially fed, and are responsible for many of these deaths. Diarrhoeal illness is also more common in artificially-fed infants even in situations with adequate hygiene, as in Belarus (23) and Scotland (24). Other acute infections, including otitis media (25), Haemophilus influenzae meningitis (26), 1 When describing age ranges, a child 6–23 months has completed 6 months but has an age less than 2 years. Source: UNICEF. Progress for children: a world fit for children. Statistical Review, Number 6. New York, UNICEF, 2007. Figure 2 Trends in exclusive breastfeeding rates (1996–2006) 0 10 20 30 40 50 0 10 20 30 40 50 Percentage of infants exclusively breastfed for the first six months of life CEE/CIS Middle East/ North Africa Sub-Saharan Africa East Asia/Pacific (excluding China) South Asia Developing countries (excluding China) around 1996 around 2006 10 19 30 26 22 30 27 32 44 45 33 37