正在加载图片...
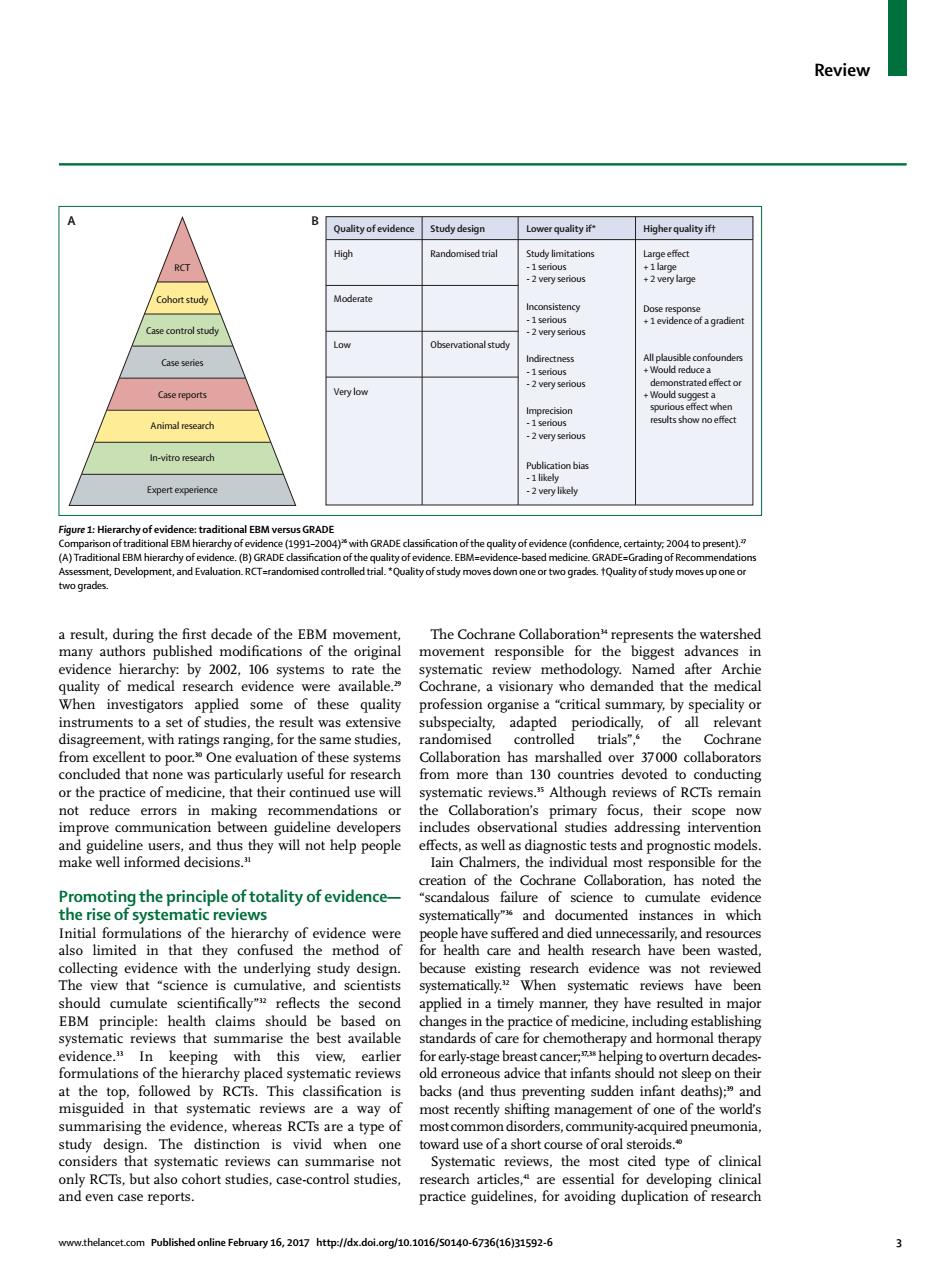
Higher qualityft in-vitro esed on bis e:traditi of the g e or two grades oves up one o 6 systems to rate review method ogy. inv estigators applied some of these qualit professi for the sames dapted h or the practice of medicine,that their continu ed use will Although reviews of RCTs remain not reduce errors in making recommendatior focus.their sts and prognost rane Collaboration.has noted th Promoting the principle of totality of evidence- scandalous science to cumuate have suffered and died unn tha the me care rch een waste The umula ave bee that summaris he best avai is of care for chemotherapy and hor ulations of the hi svste atic re old errone advice that infant on thei by ting st summarising the evid ce,whereas RC are a type of rders.commur ematic revie the most cited type of clinical but als ohort studies,case-control studies 6736(1611592-6Review www.thelancet.com Published online February 16, 2017 http://dx.doi.org/10.1016/S0140-6736(16)31592-6 3 a result, during the fi rst decade of the EBM movement, many authors published modifi cations of the original evidence hierarchy: by 2002, 106 systems to rate the quality of medical research evidence were available.29 When investigators applied some of these quality instruments to a set of studies, the result was extensive disagreement, with ratings ranging, for the same studies, from excellent to poor.30 One evaluation of these systems concluded that none was particularly useful for research or the practice of medicine, that their continued use will not reduce errors in making recommendations or improve communication between guideline developers and guideline users, and thus they will not help people make well informed decisions.31 Promoting the principle of totality of evidence— the rise of systematic reviews Initial formulations of the hierarchy of evidence were also limited in that they confused the method of collecting evidence with the underlying study design. The view that “science is cumulative, and scientists should cumulate scientifi cally”32 refl ects the second EBM principle: health claims should be based on systematic reviews that summarise the best available evidence.33 In keeping with this view, earlier formulations of the hierarchy placed systematic reviews at the top, followed by RCTs. This classifi cation is misguided in that systematic reviews are a way of summarising the evidence, whereas RCTs are a type of study design. The distinction is vivid when one considers that systematic reviews can summarise not only RCTs, but also cohort studies, case-control studies, and even case reports. The Cochrane Collaboration34 represents the watershed movement responsible for the biggest advances in systematic review methodology. Named after Archie Cochrane, a visionary who demanded that the medical profession organise a “critical summary, by speciality or subspecialty, adapted periodically, of all relevant randomised controlled trials”,6 the Cochrane Collaboration has marshalled over 37 000 collaborators from more than 130 countries devoted to conducting systematic reviews.35 Although reviews of RCTs remain the Collaboration’s primary focus, their scope now includes observational studies addressing intervention eff ects, as well as diagnostic tests and prognostic models. Iain Chalmers, the individual most responsible for the creation of the Cochrane Collaboration, has noted the “scandalous failure of science to cumulate evidence systematically”36 and documented instances in which people have suff ered and died unnecessarily, and resources for health care and health research have been wasted, because existing research evidence was not reviewed systematically.32 When systematic reviews have been applied in a timely manner, they have resulted in major changes in the practice of medicine, including establishing standards of care for chemotherapy and hormonal therapy for early-stage breast cancer;37,38 helping to overturn decadesold erroneous advice that infants should not sleep on their backs (and thus preventing sudden infant deaths);39 and most recently shifting management of one of the world’s most common disorders, community-acquired pneumonia, toward use of a short course of oral steroids.40 Systematic reviews, the most cited type of clinical research articles,41 are essential for developing clinical practice guidelines, for avoiding duplication of research RCT Cohort study Case control study Case series Case reports Animal research In-vitro research Expert experience Quality of evidence Study design Randomised trial Observational study Lower quality if* Study limitations - 1 serious - 2 very serious Inconsistency - 1 serious - 2 very serious Indirectness - 1 serious - 2 very serious Imprecision - 1 serious - 2 very serious Publication bias - 1 likely - 2 very likely Higher quality if† Large effect + 1 large + 2 very large Dose response + 1 evidence of a gradient All plausible confounders + Would reduce a demonstrated effect or + Would suggest a spurious effect when results show no effect High A B Moderate Low Very low Figure 1: Hierarchy of evidence: traditional EBM versus GRADE Comparison of traditional EBM hierarchy of evidence (1991–2004)26 with GRADE classifi cation of the quality of evidence (confi dence, certainty; 2004 to present).27 (A) Traditional EBM hierarchy of evidence. (B) GRADE classifi cation of the quality of evidence. EBM=evidence-based medicine. GRADE=Grading of Recommendations Assessment, Development, and Evaluation. RCT=randomised controlled trial. *Quality of study moves down one or two grades. †Quality of study moves up one or two grades