正在加载图片...
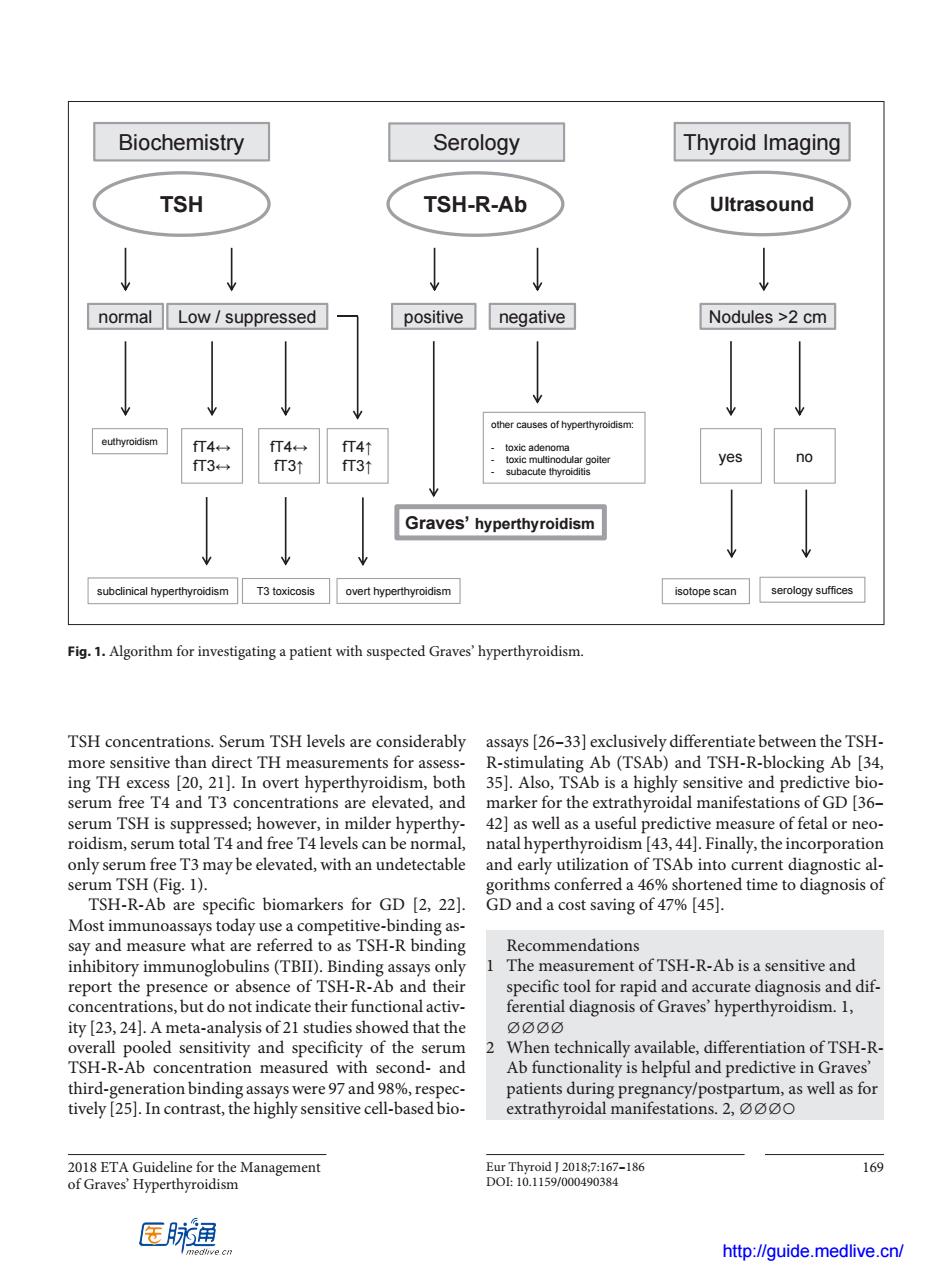
Biochemistry Serology Thyroid Imaging TSH TSH-R-Ab Ultrasound normal Low suppressed positive negative Nodules >2 cm yes no Graves'hyperthyroidism subclnical hyperthyroidism T3 toxicosis overt hyperthyroidism isotope scan serology suffices Fig1.Algorithm for investigating a patient with suspected Graveshyperthyroidism TSH concentrations.Serum TSH levels are considerably assays [26-33]exclusively differentiate between the TSH- more sensitive than direct IH measurements for asses R-stimulating Ab(TSAb)and TSH-R-blocking Ab [34, ing TH excess [20 1.Als Ab is a highly sensitive and predictive bio serun s a the extr al manifestatio hyperthy P43.44.F ffetal or ne only s ation of TSAb i al serum TSH (Fig.1. conferreda 6%shortened time to diagnosis of TSH-R-Ab are specific biomarkers for GD [2,22]. GD and a cost saving of 47%[45]. Most immunoassays today use a competitive-binding as- say and measure what are referred to as TSH-R binding Recommendations sensitive and report the pres or absence of )an specit 23.24 d that the and cificity of the tiation of TSH-R TSH-R-Ab concentration measured with second-and Ab functionality is helpful and predictive in graves third-generation binding assays were 97 and 98%.respec patients during pregnancy/postpartum,as well as for tively [25].In contrast,the highly sensitive cell-based bio- extrathyroidal manifestations.2, 16g 医肺通 http://quide medlive.cn/2018 ETA Guideline for the Management of Graves’ Hyperthyroidism Eur Thyroid J 2018;7:167–186 169 DOI: 10.1159/000490384 TSH concentrations. Serum TSH levels are considerably more sensitive than direct TH measurements for assessing TH excess [20, 21]. In overt hyperthyroidism, both serum free T4 and T3 concentrations are elevated, and serum TSH is suppressed; however, in milder hyperthyroidism, serum total T4 and free T4 levels can be normal, only serum free T3 may be elevated, with an undetectable serum TSH (Fig. 1). TSH-R-Ab are specific biomarkers for GD [2, 22]. Most immunoassays today use a competitive-binding assay and measure what are referred to as TSH-R binding inhibitory immunoglobulins (TBII). Binding assays only report the presence or absence of TSH-R-Ab and their concentrations, but do not indicate their functional activity [23, 24]. A meta-analysis of 21 studies showed that the overall pooled sensitivity and specificity of the serum TSH-R-Ab concentration measured with second- and third-generation binding assays were 97 and 98%, respectively [25]. In contrast, the highly sensitive cell-based bioassays [26–33] exclusively differentiate between the TSHR-stimulating Ab (TSAb) and TSH-R-blocking Ab [34, 35]. Also, TSAb is a highly sensitive and predictive biomarker for the extrathyroidal manifestations of GD [36– 42] as well as a useful predictive measure of fetal or neonatal hyperthyroidism [43, 44]. Finally, the incorporation and early utilization of TSAb into current diagnostic algorithms conferred a 46% shortened time to diagnosis of GD and a cost saving of 47% [45]. Recommendations 1 The measurement of TSH-R-Ab is a sensitive and specific tool for rapid and accurate diagnosis and differential diagnosis of Graves’ hyperthyroidism. 1, ∅∅∅∅ 2 When technically available, differentiation of TSH-RAb functionality is helpful and predictive in Graves’ patients during pregnancy/postpartum, as well as for extrathyroidal manifestations. 2, ∅∅∅○ Biochemistry Serology Thyroid Imaging TSH TSH-R-Ab Ultrasound normal Low / suppressed euthyroidism fT4↔ fT3↔ fT4↔ fT3↑ fT4↑ fT3↑ subclinical hyperthyroidism T3 toxicosis overt hyperthyroidism positive negative Graves’ hyperthyroidism other causes of hyperthyroidism: - toxic adenoma - toxic multinodular goiter - subacute thyroiditis Nodules >2 cm yes no isotope scan serology suffices Fig. 1. Algorithm for investigating a patient with suspected Graves’ hyperthyroidism. http://guide.medlive.cn/