正在加载图片...
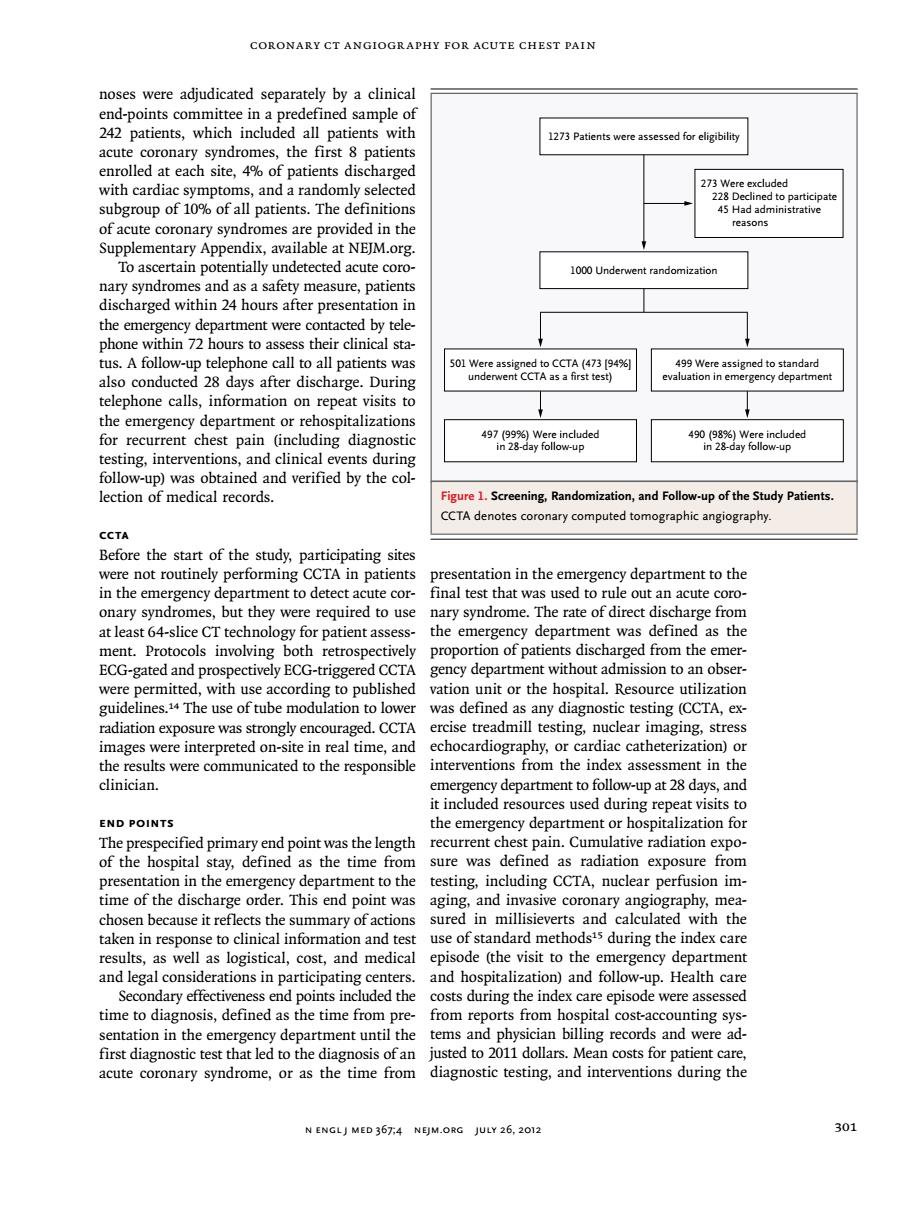
CORONARY CT ANGIOGRAPHY FOR ACUTE CHEST PAIN noses were adjudicated separately by a clinical 242 patients.which included all patients with acute coronary syndromes,the first 8 patients enrolled each site,4%o f patients dis rge with cardia ecte subgroup of patients.The ided reasons y sy To ascertain n tentially undetected acute cor 1000 Un nary syndromes and as a safety measure,patients discharged within 24 hours after presentation in the eme d by tele urs to as the ucal st tus.A fo ow-up telephone ca evongrgnopeam telenhone calls information on re at visits to the emergency department or rehospitalizations for recurrent chest pain (including diagnostic testing,interventions,and clinical nts during the 1.Screening.Randomizatio and Folt up of the Study Patien coronary compu angiograph CCTA Before the start of the study.participating site were not routinely performing CCTA in patients presentation in the emergency department to the in the emergency department to detect acute cor- final test that was used to rule out an acute coro- onary syndromes,but they were required to use nary syndrome.The rate of direct discharge fron at least 64-slic for patient as the em t wa as th mitte with use accordin vation unit or the hospital.Resource utilization guidelines.The use of tube modulation to lower was defined as any diagnostic testing (CcTa ex- radiation exposure was strongly encouraged.CCTA ercise treadmill testing,nuclear imaging,stress images were interpreted on-site in real time,and echocardiography,or cardiac catheterization)or interventions from the ent in th y department to v-up at 28 END POINTS cu der The pr pecified primary end point was the le recurrent chest pain.Cumulative radiation expo sure was defined as radiation exposure from presentation in the emergency department to the testing,including CCTA,nuclear perfusion im- time of the discharge order.This end point was aging,and in sive coronary angiography,me chosen because it re ts th of act e St sure thth taken in respo dur to the degal consider tio s in n and ho pitalization)and fol Health Secondary effective ness end points included the costs during the index care episode were assessed time to diagnosis.defined as the time from pre from reports from hospital cost-accounting sys sentation in the emergency department until the tems and physician billing records and were ad first diagnostic test that led to the diagnosis of an ted to 2011 ars. n costs to acute coronary synd rome,or as the time fror diagnostic testing,and inte ventions ring th N ENGLJ MED 367:4 NEJM.ORG JULY 26,2012 301coronary CT Angiogr aphy for Acute Chest Pain n engl j med 367;4 nejm.org july 26, 2012 301 noses were adjudicated separately by a clinical end-points committee in a predefined sample of 242 patients, which included all patients with acute coronary syndromes, the first 8 patients enrolled at each site, 4% of patients discharged with cardiac symptoms, and a randomly selected subgroup of 10% of all patients. The definitions of acute coronary syndromes are provided in the Supplementary Appendix, available at NEJM.org. To ascertain potentially undetected acute coronary syndromes and as a safety measure, patients discharged within 24 hours after presentation in the emergency department were contacted by telephone within 72 hours to assess their clinical status. A follow-up telephone call to all patients was also conducted 28 days after discharge. During telephone calls, information on repeat visits to the emergency department or rehospitalizations for recurrent chest pain (including diagnostic testing, interventions, and clinical events during follow-up) was obtained and verified by the collection of medical records. CCTA Before the start of the study, participating sites were not routinely performing CCTA in patients in the emergency department to detect acute coronary syndromes, but they were required to use at least 64-slice CT technology for patient assessment. Protocols involving both retrospectively ECG-gated and prospectively ECG-triggered CCTA were permitted, with use according to published guidelines.14 The use of tube modulation to lower radiation exposure was strongly encouraged. CCTA images were interpreted on-site in real time, and the results were communicated to the responsible clinician. End Points The prespecified primary end point was the length of the hospital stay, defined as the time from presentation in the emergency department to the time of the discharge order. This end point was chosen because it reflects the summary of actions taken in response to clinical information and test results, as well as logistical, cost, and medical and legal considerations in participating centers. Secondary effectiveness end points included the time to diagnosis, defined as the time from presentation in the emergency department until the first diagnostic test that led to the diagnosis of an acute coronary syndrome, or as the time from presentation in the emergency department to the final test that was used to rule out an acute coronary syndrome. The rate of direct discharge from the emergency department was defined as the proportion of patients discharged from the emergency department without admission to an observation unit or the hospital. Resource utilization was defined as any diagnostic testing (CCTA, exercise treadmill testing, nuclear imaging, stress echocardiography, or cardiac catheterization) or interventions from the index assessment in the emergency department to follow-up at 28 days, and it included resources used during repeat visits to the emergency department or hospitalization for recurrent chest pain. Cumulative radiation exposure was defined as radiation exposure from testing, including CCTA, nuclear perfusion imaging, and invasive coronary angiography, measured in millisieverts and calculated with the use of standard methods15 during the index care episode (the visit to the emergency department and hospitalization) and follow-up. Health care costs during the index care episode were assessed from reports from hospital cost-accounting systems and physician billing records and were adjusted to 2011 dollars. Mean costs for patient care, diagnostic testing, and interventions during the 1000 Underwent randomization 1273 Patients were assessed for eligibility 273 Were excluded 228 Declined to participate 45 Had administrative reasons 501 Were assigned to CCTA (473 [94%] underwent CCTA as a first test) 499 Were assigned to standard evaluation in emergency department 497 (99%) Were included in 28-day follow-up 490 (98%) Were included in 28-day follow-up Figure 1. Screening, Randomization, and Follow-up of the Study Patients. CCTA denotes coronary computed tomographic angiography