正在加载图片...
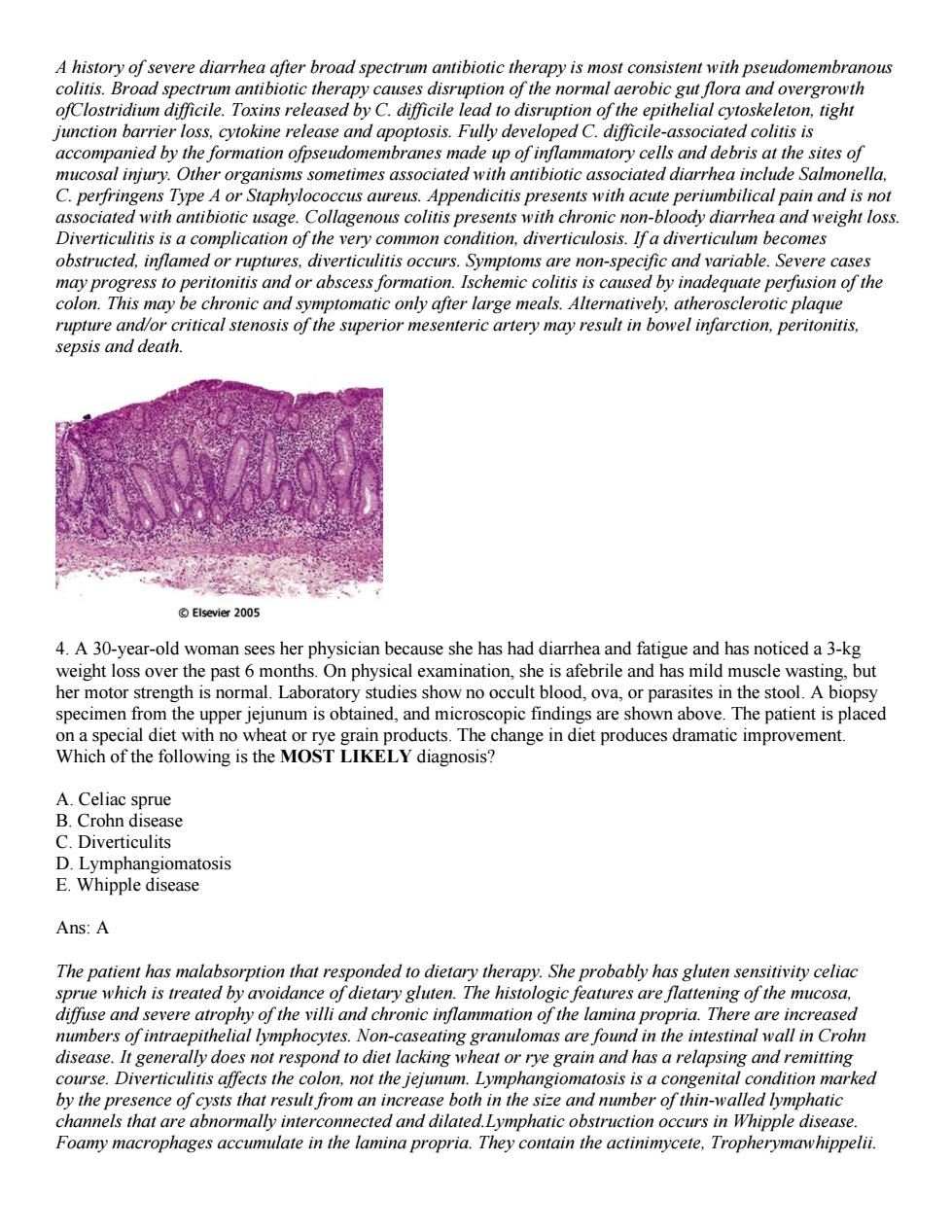
wmo of the normo overgrowth eleton,tight junction barrier loss,cytokine release and apoptosis.Fully developed C.difficile-associated colitis is accompanied by the formation ofpseudomembranes made up of inflammatory cells and debris at the sites of mucosal injury.Other organisms sometimes associated with antibiotic associated diarrhea include Salmonella. C.perfringens Type A or Staphylococcus aureus.Appendicitis presents with acute periumbilical pain and is not associated with antibiotic usage.Collagenous colitis presents with chronic non-bloody diarrhea and weight loss Diverticulitis is a complication of the very common condition,diverticulosis.If a diverticulum becomes obstructed,inflamed or ruptures,diverticulitis occurs.Symptoms are non-specific and variable.Severe cases may progress to peritonitis and or abscess formation.Ischemic colitis is caused by inadequate perfusion of the colon.This may be chronic and symptomatic only after large meals.Alternatively,atherosclerotic plaque rupture and/or critical stenosis of the superior mesenteric artery may result in bowel infarction,peritonitis. sepsis and death. 4.A 30-year-old woman sees her physician because she has had diarrhea and fatigue and has noticed a 3-kg weight loss over the past 6 months.On physical examination,she is afebrile and has mild muscle wasting,but her motor strength is normal.Laborator studies show no occult blood.ova.or parasites in the stool.A bior speci en fr the u show above cial diet with no .The patient ispla at following is the MOSTLIKELY hange in die et produces c improvement diagnosis Lymphangiomatosis E.Whipple disease Ans:A The patient has malabsorption that responded to dietary therapy.She probably has gluten sensitivity celiac sprue which is treated by avoidance of dietary gluten.The histologic features are flattening of the mucosa. diffuse and severe atrophy of the villi and chronic inflammation of the lamina propria.There are increased numbers of intraepithelial lymphocytes.Non-caseating granulomas are found in the intestinal wall in Crohn disease.It generally does not respond to diet lacking wheat or rye grain and has a relapsing and remitting course.Diverticulitis affects the colon,not the jejunum.Lymphangiomatosis is a cong nital condition marked se both in the s sie and number of thin-walled lymphatic are abno ole disease Foamy macrophages ac ate in the lamina proprig.They conain the acinnneete. rymawhippelii.A history of severe diarrhea after broad spectrum antibiotic therapy is most consistent with pseudomembranous colitis. Broad spectrum antibiotic therapy causes disruption of the normal aerobic gut flora and overgrowth ofClostridium difficile. Toxins released by C. difficile lead to disruption of the epithelial cytoskeleton, tight junction barrier loss, cytokine release and apoptosis. Fully developed C. difficile-associated colitis is accompanied by the formation ofpseudomembranes made up of inflammatory cells and debris at the sites of mucosal injury. Other organisms sometimes associated with antibiotic associated diarrhea include Salmonella, C. perfringens Type A or Staphylococcus aureus. Appendicitis presents with acute periumbilical pain and is not associated with antibiotic usage. Collagenous colitis presents with chronic non-bloody diarrhea and weight loss. Diverticulitis is a complication of the very common condition, diverticulosis. If a diverticulum becomes obstructed, inflamed or ruptures, diverticulitis occurs. Symptoms are non-specific and variable. Severe cases may progress to peritonitis and or abscess formation. Ischemic colitis is caused by inadequate perfusion of the colon. This may be chronic and symptomatic only after large meals. Alternatively, atherosclerotic plaque rupture and/or critical stenosis of the superior mesenteric artery may result in bowel infarction, peritonitis, sepsis and death. 4. A 30-year-old woman sees her physician because she has had diarrhea and fatigue and has noticed a 3-kg weight loss over the past 6 months. On physical examination, she is afebrile and has mild muscle wasting, but her motor strength is normal. Laboratory studies show no occult blood, ova, or parasites in the stool. A biopsy specimen from the upper jejunum is obtained, and microscopic findings are shown above. The patient is placed on a special diet with no wheat or rye grain products. The change in diet produces dramatic improvement. Which of the following is the MOST LIKELY diagnosis? A. Celiac sprue B. Crohn disease C. Diverticulits D. Lymphangiomatosis E. Whipple disease Ans: A The patient has malabsorption that responded to dietary therapy. She probably has gluten sensitivity celiac sprue which is treated by avoidance of dietary gluten. The histologic features are flattening of the mucosa, diffuse and severe atrophy of the villi and chronic inflammation of the lamina propria. There are increased numbers of intraepithelial lymphocytes. Non-caseating granulomas are found in the intestinal wall in Crohn disease. It generally does not respond to diet lacking wheat or rye grain and has a relapsing and remitting course. Diverticulitis affects the colon, not the jejunum. Lymphangiomatosis is a congenital condition marked by the presence of cysts that result from an increase both in the size and number of thin-walled lymphatic channels that are abnormally interconnected and dilated.Lymphatic obstruction occurs in Whipple disease. Foamy macrophages accumulate in the lamina propria. They contain the actinimycete, Tropherymawhippelii