正在加载图片...
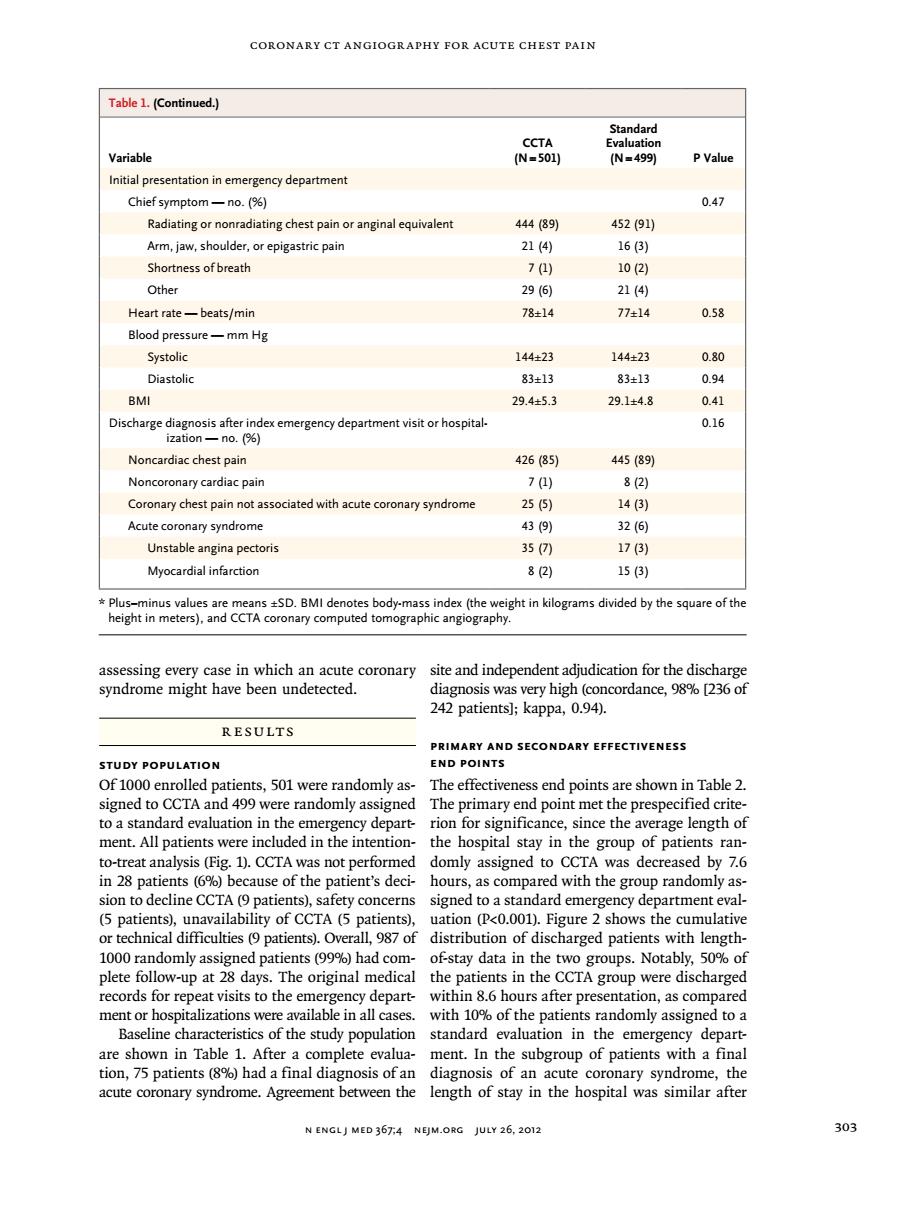
CORONARY CT ANGIOGRAPHY FOR ACUTE CHEST PAIN Table 1.(Continued.) ( PValu Initial presentation in emergency departmen Chief symptom一no.%) 0.47 Radiating or nonradiating chest pain or anginal equivalent 44489 452(91) Arm,jaw,shoulder.or epigastric pain 2】14 163) Shortness of breath 71 102 Other Heart rate-beats/min 0.58 Blood pressure一mmHe Systolic 144±23 144±23 Diastolic 83±13 83±13 0.94 RMI 29.4±5.3 29.1±4.8 041 0.16 Noncardiac chest pain 426(85 445(89 Noncoronary cardiac pair 71) 8(2) Coronary chest pain not asso with syndrome 255 1431 Acute syndrome 9) 32(同 Unstable angina pectori 35 Myocardial infarction 82) 15(3) sSD.BMI denotes body-mass index(the om ded byeof in which coronary site and inder enden adjudication for the disch ordanc, 242 patients]:kappa,0.94). RESULTS PRIMARY A STUDY POPUL Of100 e ts,501were randomly a e effectiv end points are shown in Table2. toed to domy a: ndard evalua since the ment.All patients were included in the inte the hospital stay in the group of patients ran- to-treat analysis (Fig.1).CCTA was not performed domly assigned to CCTA was decreased by 7.6 in 28 patients(6%)because of the patient's deci-hours,as compared with the group randomly as- patients),safety concerns signed to a sta dard emergency de partment eval ty or CCIA (5 pa .00 ws th 1000 The riginal medical the atients in th ere disch records for repeat visits to the eme gency depart-within 86 hours after presentation as comp red ment or hospitalizations were available inall cases.with 10%of the patients randomly assigned toa Baseline charact eristics of the study population standard evaluation in the emergen depart are shown in Table 1 After a complete evalua- ment.In the subgroup of patients with a fina final or an cor Agreement between the N ENGLJ MED 367:4 NEJM.ORG JULY 26,2012coronary CT Angiogr aphy for Acute Chest Pain n engl j med 367;4 nejm.org july 26, 2012 303 assessing every case in which an acute coronary syndrome might have been undetected. R esult s Study Population Of 1000 enrolled patients, 501 were randomly assigned to CCTA and 499 were randomly assigned to a standard evaluation in the emergency department. All patients were included in the intentionto-treat analysis (Fig. 1). CCTA was not performed in 28 patients (6%) because of the patient’s decision to decline CCTA (9 patients), safety concerns (5 patients), unavailability of CCTA (5 patients), or technical difficulties (9 patients). Overall, 987 of 1000 randomly assigned patients (99%) had complete follow-up at 28 days. The original medical records for repeat visits to the emergency department or hospitalizations were available in all cases. Baseline characteristics of the study population are shown in Table 1. After a complete evaluation, 75 patients (8%) had a final diagnosis of an acute coronary syndrome. Agreement between the site and independent adjudication for the discharge diagnosis was very high (concordance, 98% [236 of 242 patients]; kappa, 0.94). Primary and Secondary Effectiveness End Points The effectiveness end points are shown in Table 2. The primary end point met the prespecified criterion for significance, since the average length of the hospital stay in the group of patients randomly assigned to CCTA was decreased by 7.6 hours, as compared with the group randomly assigned to a standard emergency department evaluation (P<0.001). Figure 2 shows the cumulative distribution of discharged patients with lengthof-stay data in the two groups. Notably, 50% of the patients in the CCTA group were discharged within 8.6 hours after presentation, as compared with 10% of the patients randomly assigned to a standard evaluation in the emergency department. In the subgroup of patients with a final diagnosis of an acute coronary syndrome, the length of stay in the hospital was similar after Table 1. (Continued.) Variable CCTA (N=501) Standard Evaluation (N=499) P Value Initial presentation in emergency department Chief symptom — no. (%) 0.47 Radiating or nonradiating chest pain or anginal equivalent 444 (89) 452 (91) Arm, jaw, shoulder, or epigastric pain 21 (4) 16 (3) Shortness of breath 7 (1) 10 (2) Other 29 (6) 21 (4) Heart rate — beats/min 78±14 77±14 0.58 Blood pressure — mm Hg Systolic 144±23 144±23 0.80 Diastolic 83±13 83±13 0.94 BMI 29.4±5.3 29.1±4.8 0.41 Discharge diagnosis after index emergency department visit or hospitalization — no. (%) 0.16 Noncardiac chest pain 426 (85) 445 (89) Noncoronary cardiac pain 7 (1) 8 (2) Coronary chest pain not associated with acute coronary syndrome 25 (5) 14 (3) Acute coronary syndrome 43 (9) 32 (6) Unstable angina pectoris 35 (7) 17 (3) Myocardial infarction 8 (2) 15 (3) * Plus–minus values are means ±SD. BMI denotes body-mass index (the weight in kilograms divided by the square of the height in meters), and CCTA coronary computed tomographic angiography