正在加载图片...
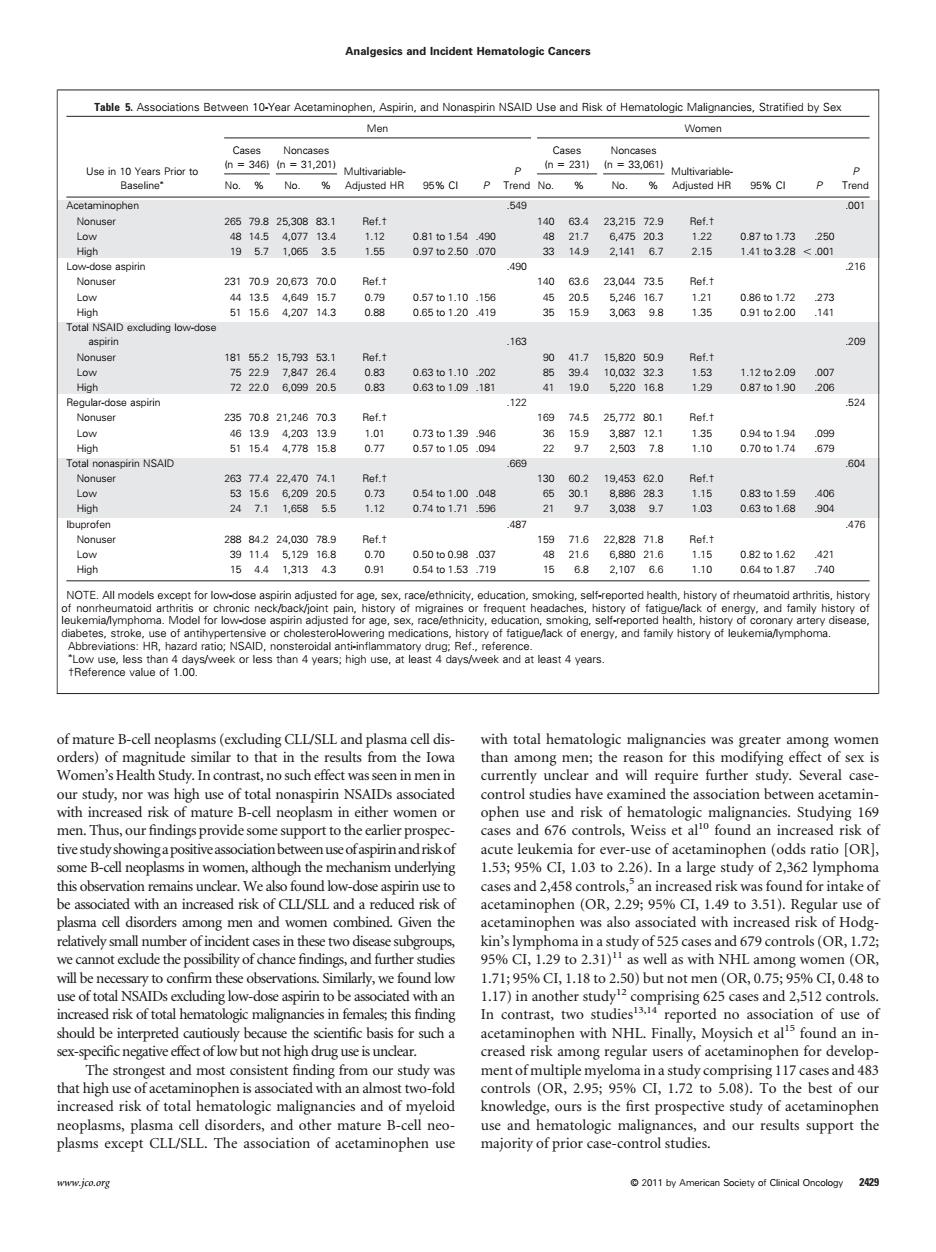
Analgesics and Incident Hematologic Cancers Table 5.Associations Between 10-Year Acetaminophen,Aspirin,and Nonaspirin NSAID Use and Risk of Hematologic Matgnancies,Stratified by Sex Men No.%No.. No.No. he 19571,0653.5 1.55 2.16 40 216 886 o .163 20 819 -122 甜 16974.5257720 881 1.12 888 050to0.9037 1544131343 0.91 054o153719 156.82,1076.6 1.10 NOTE.All m dat east4years was greater among womer Women's Heath Study.In contrast,no such effect currently undear and will require further study.Several case ud水.nor u women0 .03 to be assoated with increasedisk of CL/SLand a reducedisk of acetaminophen (OR.%Cl,1.9 to 3.51).Regular use of velyude the rof in ary to confirm these ob vations Similarly.we found low 1.71:95%CL,1.18to2.50)but not men(0R,0.75,95%CL,0.48t0 17刀nnotherucapring625aeind3l2oatob sex-specificnegative effect of low but not high drug use is undear. among regula users of acetaminophen for develop 40 knowledge.ours is the first pros ective study of acetaminophen use and hematologic malignances,and our results support the The association of acetaminophen use majority of prior case-control studies www.jco.org 2011yof mature B-cell neoplasms (excluding CLL/SLL and plasma cell disorders) of magnitude similar to that in the results from the Iowa Women’s Health Study. In contrast, no such effect was seen in men in our study, nor was high use of total nonaspirin NSAIDs associated with increased risk of mature B-cell neoplasm in either women or men. Thus, our findings provide some support to the earlier prospective study showingapositiveassociationbetweenuseofaspirinand riskof some B-cell neoplasms in women, although the mechanism underlying this observation remains unclear. We also found low-dose aspirin use to be associated with an increased risk of CLL/SLL and a reduced risk of plasma cell disorders among men and women combined. Given the relatively small number of incident cases in these two disease subgroups, we cannot exclude the possibility of chance findings, and further studies will be necessary to confirm these observations. Similarly, we found low use of total NSAIDs excluding low-dose aspirin to be associated with an increased risk of total hematologic malignancies in females; this finding should be interpreted cautiously because the scientific basis for such a sex-specific negative effect of low but not high drug use is unclear. The strongest and most consistent finding from our study was that high use of acetaminophen is associated with an almost two-fold increased risk of total hematologic malignancies and of myeloid neoplasms, plasma cell disorders, and other mature B-cell neoplasms except CLL/SLL. The association of acetaminophen use with total hematologic malignancies was greater among women than among men; the reason for this modifying effect of sex is currently unclear and will require further study. Several casecontrol studies have examined the association between acetaminophen use and risk of hematologic malignancies. Studying 169 cases and 676 controls, Weiss et al10 found an increased risk of acute leukemia for ever-use of acetaminophen (odds ratio [OR], 1.53; 95% CI, 1.03 to 2.26). In a large study of 2,362 lymphoma cases and 2,458 controls,5 an increased risk was found for intake of acetaminophen (OR, 2.29; 95% CI, 1.49 to 3.51). Regular use of acetaminophen was also associated with increased risk of Hodgkin’s lymphoma in a study of 525 cases and 679 controls (OR, 1.72; 95% CI, 1.29 to 2.31)11 as well as with NHL among women (OR, 1.71; 95% CI, 1.18 to 2.50) but not men (OR, 0.75; 95% CI, 0.48 to 1.17) in another study12 comprising 625 cases and 2,512 controls. In contrast, two studies13,14 reported no association of use of acetaminophen with NHL. Finally, Moysich et al15 found an increased risk among regular users of acetaminophen for development of multiple myeloma in a study comprising 117 cases and 483 controls (OR, 2.95; 95% CI, 1.72 to 5.08). To the best of our knowledge, ours is the first prospective study of acetaminophen use and hematologic malignances, and our results support the majority of prior case-control studies. Table 5. Associations Between 10-Year Acetaminophen, Aspirin, and Nonaspirin NSAID Use and Risk of Hematologic Malignancies, Stratified by Sex Use in 10 Years Prior to Baseline Men Women Cases (n 346) Noncases (n 31,201) MultivariableAdjusted HR 95% CI P P Trend Cases (n 231) Noncases (n 33,061) MultivariableAdjusted HR 95% CI P P No. % No. % No. % No. % Trend Acetaminophen .549 .001 Nonuser 265 79.8 25,308 83.1 Ref.† 140 63.4 23,215 72.9 Ref.† Low 48 14.5 4,077 13.4 1.12 0.81 to 1.54 .490 48 21.7 6,475 20.3 1.22 0.87 to 1.73 .250 High 19 5.7 1,065 3.5 1.55 0.97 to 2.50 .070 33 14.9 2,141 6.7 2.15 1.41 to 3.28 .001 Low-dose aspirin .490 .216 Nonuser 231 70.9 20,673 70.0 Ref.† 140 63.6 23,044 73.5 Ref.† Low 44 13.5 4,649 15.7 0.79 0.57 to 1.10 .156 45 20.5 5,246 16.7 1.21 0.86 to 1.72 .273 High 51 15.6 4,207 14.3 0.88 0.65 to 1.20 .419 35 15.9 3,063 9.8 1.35 0.91 to 2.00 .141 Total NSAID excluding low-dose aspirin .163 .209 Nonuser 181 55.2 15,793 53.1 Ref.† 90 41.7 15,820 50.9 Ref.† Low 75 22.9 7,847 26.4 0.83 0.63 to 1.10 .202 85 39.4 10,032 32.3 1.53 1.12 to 2.09 .007 High 72 22.0 6,099 20.5 0.83 0.63 to 1.09 .181 41 19.0 5,220 16.8 1.29 0.87 to 1.90 .206 Regular-dose aspirin .122 .524 Nonuser 235 70.8 21,246 70.3 Ref.† 169 74.5 25,772 80.1 Ref.† Low 46 13.9 4,203 13.9 1.01 0.73 to 1.39 .946 36 15.9 3,887 12.1 1.35 0.94 to 1.94 .099 High 51 15.4 4,778 15.8 0.77 0.57 to 1.05 .094 22 9.7 2,503 7.8 1.10 0.70 to 1.74 .679 Total nonaspirin NSAID .669 .604 Nonuser 263 77.4 22,470 74.1 Ref.† 130 60.2 19,453 62.0 Ref.† Low 53 15.6 6,209 20.5 0.73 0.54 to 1.00 .048 65 30.1 8,886 28.3 1.15 0.83 to 1.59 .406 High 24 7.1 1,658 5.5 1.12 0.74 to 1.71 .596 21 9.7 3,038 9.7 1.03 0.63 to 1.68 .904 Ibuprofen .487 .476 Nonuser 288 84.2 24,030 78.9 Ref.† 159 71.6 22,828 71.8 Ref.† Low 39 11.4 5,129 16.8 0.70 0.50 to 0.98 .037 48 21.6 6,880 21.6 1.15 0.82 to 1.62 .421 High 15 4.4 1,313 4.3 0.91 0.54 to 1.53 .719 15 6.8 2,107 6.6 1.10 0.64 to 1.87 .740 NOTE. All models except for low-dose aspirin adjusted for age, sex, race/ethnicity, education, smoking, self-reported health, history of rheumatoid arthritis, history of nonrheumatoid arthritis or chronic neck/back/joint pain, history of migraines or frequent headaches, history of fatigue/lack of energy, and family history of leukemia/lymphoma. Model for low-dose aspirin adjusted for age, sex, race/ethnicity, education, smoking, self-reported health, history of coronary artery disease, diabetes, stroke, use of antihypertensive or cholesterol-lowering medications, history of fatigue/lack of energy, and family history of leukemia/lymphoma. Abbreviations: HR, hazard ratio; NSAID, nonsteroidal anti-inflammatory drug; Ref., reference. Low use, less than 4 days/week or less than 4 years; high use, at least 4 days/week and at least 4 years. †Reference value of 1.00. Analgesics and Incident Hematologic Cancers www.jco.org © 2011 by American Society of Clinical Oncology 2429�