正在加载图片...
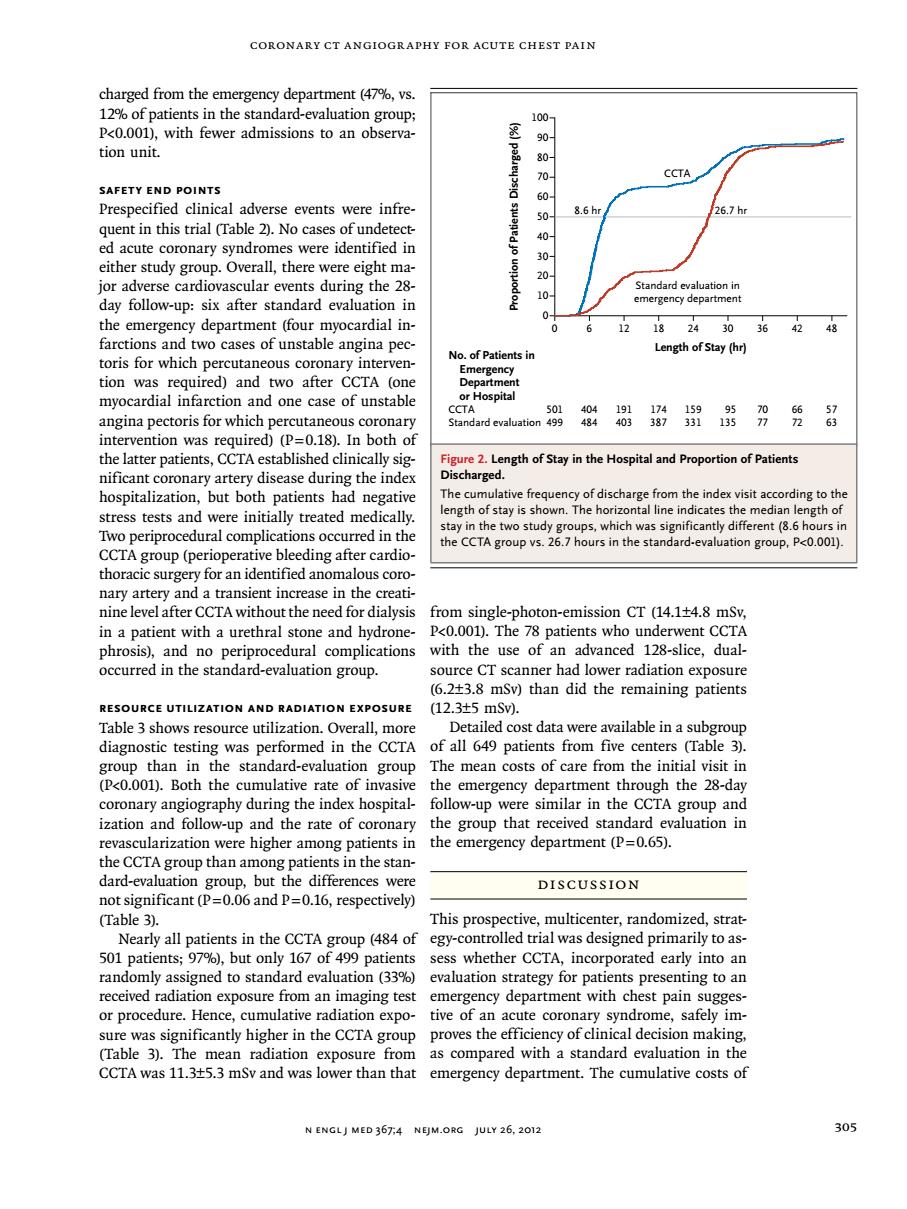
CORONARY CT ANGIOGRAPHY FOR ACUTE CHEST PAIN charged from the emerg ncy depa ment (47 vs 12%of patients in the standard. pcoool.witfeweradmisionsonobo tion unit. CCTA Prespe cal adverse events were nfre 86 6.7h jor adverse cardiovascular events during the 28- day follow-up:six after standard evaluation in the emergency department (four myocardial in- 6 1218240364248 two cases of unstable angina pec Length ofStay (hr) of P mvocardial infarction and one case of unstable angina pectoris for which percutaneous coronary intervention was required)(P=0.18).In both of the latter patients,CCTA established clinically sig Length of Stay in the Hospital and Proporion of Patients tive fregu cy of dischar e from the index visit according to th ress tests ted me ngth of stay is shown.The hori ngth c CCTA the CCTA group vs.2 rdio. .thestandard-evaigroP01) thoracic surgery for an identified anomalous coro nary artery and a transient increase in the creati nine level after CCTA without the need for dialysis in a patient wit a urethra stone and hydrone vith adi RESOURCE UTILIZATION AND RADIATION EXPOSURE (12.3t5mSv. Table 3 shows resource utilization.Overall,more Detailed cost data were available in a subgroup diagnostic testing was performed in the CCTA of all 649 patients from five centers (Table 3 e standard-evaluation group The mean costs of care from the initial visit i the emergency dep ent throug n the 28 nd the the the CCTA group than among patients in the stan- dard-evaluation group,but the differences were DISCUSSION not significant(P=0.06 and P=0.16,respectively) (Table 3). strat Nearly all patients in the CC T This to a ,1 oup(484 of egy-contro ed to stand sation str received radiation exposure from an imaging test emergency department with chest pain sugges- or procedure.Hence,cumulative radiation expo-tive of an acute coronary syndrome,safely im- sure was significantly higher in the CCTA group proves the efficiency of clinical decision making (Table 3).The mean radiation exposure fron as compared with a standard eva ation in the CCTA was 11.3+5.3 mSv and was lower than that emergency department.The cumulative costs of N ENGLJ MED 367:4 NEJM.ORG JULY 26,2012 305coronary CT Angiogr aphy for Acute Chest Pain n engl j med 367;4 nejm.org july 26, 2012 305 charged from the emergency department (47%, vs. 12% of patients in the standard-evaluation group; P<0.001), with fewer admissions to an observation unit. Safety End Points Prespecified clinical adverse events were infrequent in this trial (Table 2). No cases of undetected acute coronary syndromes were identified in either study group. Overall, there were eight major adverse cardiovascular events during the 28- day follow-up: six after standard evaluation in the emergency department (four myocardial infarctions and two cases of unstable angina pectoris for which percutaneous coronary intervention was required) and two after CCTA (one myocardial infarction and one case of unstable angina pectoris for which percutaneous coronary intervention was required) (P=0.18). In both of the latter patients, CCTA established clinically significant coronary artery disease during the index hospitalization, but both patients had negative stress tests and were initially treated medically. Two periprocedural complications occurred in the CCTA group (perioperative bleeding after cardiothoracic surgery for an identified anomalous coronary artery and a transient increase in the creatinine level after CCTA without the need for dialysis in a patient with a urethral stone and hydronephrosis), and no periprocedural complications occurred in the standard-evaluation group. Resource Utilization and Radiation Exposure Table 3 shows resource utilization. Overall, more diagnostic testing was performed in the CCTA group than in the standard-evaluation group (P<0.001). Both the cumulative rate of invasive coronary angiography during the index hospitalization and follow-up and the rate of coronary revascularization were higher among patients in the CCTA group than among patients in the standard-evaluation group, but the differences were not significant (P=0.06 and P=0.16, respectively) (Table 3). Nearly all patients in the CCTA group (484 of 501 patients; 97%), but only 167 of 499 patients randomly assigned to standard evaluation (33%) received radiation exposure from an imaging test or procedure. Hence, cumulative radiation exposure was significantly higher in the CCTA group (Table 3). The mean radiation exposure from CCTA was 11.3±5.3 mSv and was lower than that from single-photon-emission CT (14.1±4.8 mSv, P<0.001). The 78 patients who underwent CCTA with the use of an advanced 128-slice, dualsource CT scanner had lower radiation exposure (6.2±3.8 mSv) than did the remaining patients (12.3±5 mSv). Detailed cost data were available in a subgroup of all 649 patients from five centers (Table 3). The mean costs of care from the initial visit in the emergency department through the 28-day follow-up were similar in the CCTA group and the group that received standard evaluation in the emergency department (P=0.65). Discussion This prospective, multicenter, randomized, strategy-controlled trial was designed primarily to assess whether CCTA, incorporated early into an evaluation strategy for patients presenting to an emergency department with chest pain suggestive of an acute coronary syndrome, safely improves the efficiency of clinical decision making, as compared with a standard evaluation in the emergency department. The cumulative costs of Proportion of Patients Discharged (%) 100 80 90 70 60 40 30 10 50 20 0 0 6 12 18 24 30 36 42 48 Length of Stay (hr) No. of Patients in Emergency Department or Hospital CCTA Standard evaluation 501 499 404 484 174 387 191 403 159 331 95 135 66 72 70 77 57 63 CCTA Standard evaluation in emergency department 8.6 hr 26.7 hr Figure 2. Length of Stay in the Hospital and Proportion of Patients Discharged. The cumulative frequency of discharge from the index visit according to the length of stay is shown. The horizontal line indicates the median length of stay in the two study groups, which was significantly different (8.6 hours in the CCTA group vs. 26.7 hours in the standard-evaluation group, P<0.001)