正在加载图片...
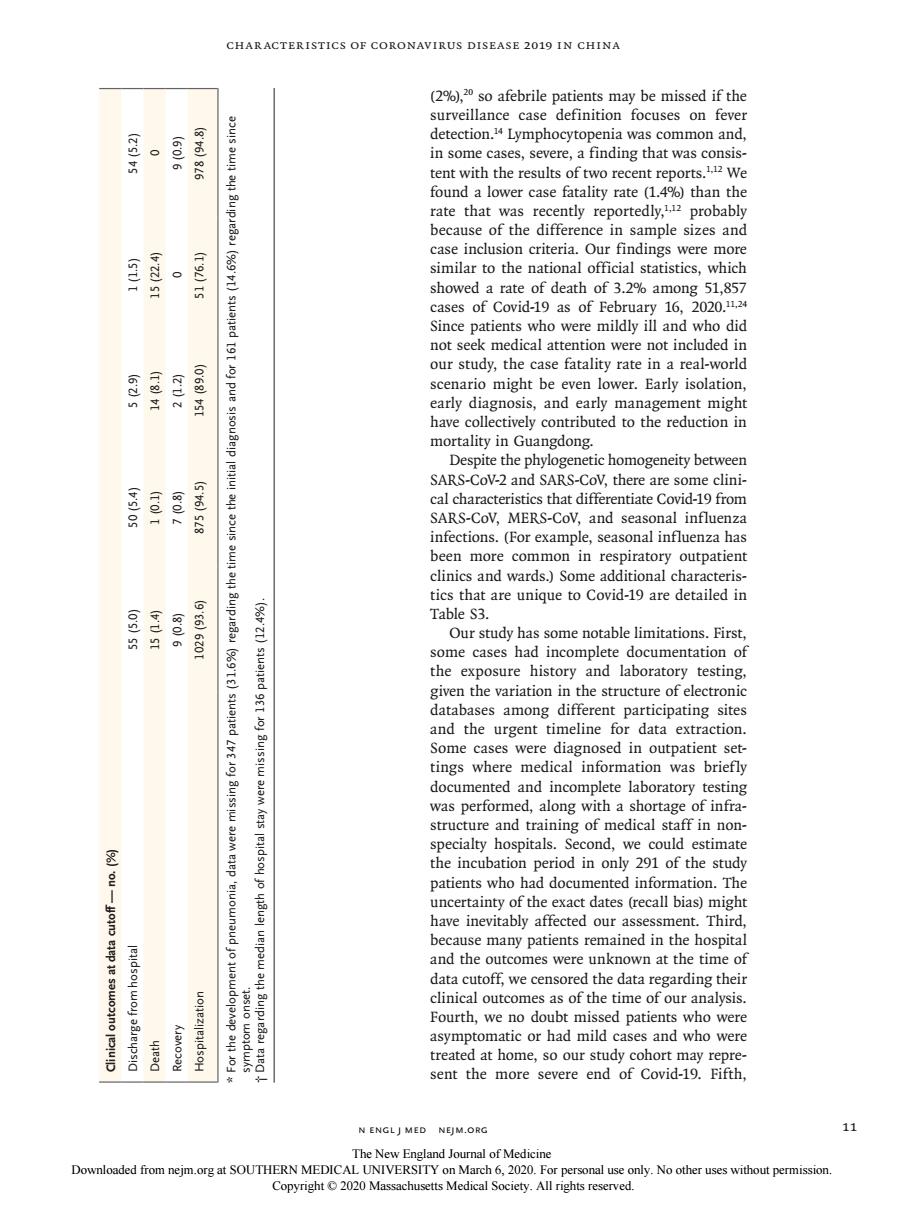
CHARACTERISTICS OF CORONAVIRUS DISEASE 2019 IN CHINA (2%)20 so afebrile patients may be missed if the surveillance case definition focuses on fever detection.Lymphocytopenia was common and, in some cases,severe,a finding that was consis tent with the results of two recent reports. because of the difference in sample sizes and case inclusion criteria our findings were more similar to the national official statistics,which showed a rate of death of 3.2%among 51,857 cases of Covid- 9 as of F 20. atenoti pue sisou scenario might be even lower.Early isolation early diagnosis,and early management might have collectively contributed to the reduction in mortality in Guangdong. omogeneity betv 明 uariplpitluialaaau and SA SARS-COV.MERS-CoV. and se infections (for example seasonal influenza has been more common in respiratory outpatient clinics and wards.)Some additional characteris- aren to Cov-are detailedin le S3 had ete do the exnosure history and laboratory testing sualtrdSEtOsaulBluuaiaMestTdwoloBuaVEPgu emeer n and the urgent timeline for data extraction Some cases were dical d1 ed alo structure and training of medical staff in non specialty hospitals.Second,we could estimate the incubation period in only 291 of the study patients who had documented information.The and the outcomes were unknown at the time of data cutoff we censored the data regarding their clinical outcomes as of the time of our analysis. the N ENGLJ MED NEJM.ORG 11 The New Engl land Journal of Medicine n engl j med nejm.org 11 Char acteristics of Coronavirus Disease 2019 in China (2%),20 so afebrile patients may be missed if the surveillance case definition focuses on fever detection.14 Lymphocytopenia was common and, in some cases, severe, a finding that was consis - tent with the results of two recent reports.1,12 We found a lower case fatality rate (1.4%) than the rate that was recently reportedly,1,12 probably because of the difference in sample sizes and case inclusion criteria. Our findings were more similar to the national official statistics, which showed a rate of death of 3.2% among 51,857 cases of Covid-19 as of February 16, 2020.11,24 Since patients who were mildly ill and who did not seek medical attention were not included in our study, the case fatality rate in a real-world scenario might be even lower. Early isolation, early diagnosis, and early management might have collectively contributed to the reduction in mortality in Guangdong. Despite the phylogenetic homogeneity between SARS-CoV-2 and SARS-CoV, there are some clini - cal characteristics that differentiate Covid-19 from SARS-CoV, MERS-CoV, and seasonal influenza infections. (For example, seasonal influenza has been more common in respiratory outpatient clinics and wards.) Some additional characteris - tics that are unique to Covid-19 are detailed in Table S3. Our study has some notable limitations. First, some cases had incomplete documentation of the exposure history and laboratory testing, given the variation in the structure of electronic databases among different participating sites and the urgent timeline for data extraction. Some cases were diagnosed in outpatient settings where medical information was briefly documented and incomplete laboratory testing was performed, along with a shortage of infra - structure and training of medical staff in non - specialty hospitals. Second, we could estimate the incubation period in only 291 of the study patients who had documented information. The uncertainty of the exact dates (recall bias) might have inevitably affected our assessment. Third, because many patients remained in the hospital and the outcomes were unknown at the time of data cutoff, we censored the data regarding their clinical outcomes as of the time of our analysis. Fourth, we no doubt missed patients who were asymptomatic or had mild cases and who were treated at home, so our study cohort may repre - sent the more severe end of Covid-19. Fifth, Variable All Patients (N=1099) Disease Severity Presence of Composite Primary End Point Nonsevere (N=926) Severe (N=173) Yes (N=67) No (N=1032) Clinical outcomes at data cutoff — no. (%) Discharge from hospital 55 (5.0) 50 (5.4) 5 (2.9) 1 (1.5) 54 (5.2) Death 15 (1.4) 1 (0.1) 14 (8.1) 15 (22.4) 0 Recovery 9 (0.8) 7 (0.8) 2 (1.2) 0 9 (0.9) Hospitalization 1029 (93.6) 875 (94.5) 154 (89.0) 51 (76.1) 978 (94.8) * For the development of pneumonia, data were missing for 347 patients (31.6%) regarding the time since the initial diagnosis and for 161 patients (14.6%) regarding the time since symptom onset. † Data regarding the median length of hospital stay were missing for 136 patients (12.4%). The New England Journal of Medicine Downloaded from nejm.org at SOUTHERN MEDICAL UNIVERSITY on March 6, 2020. For personal use only. No other uses without permission. Copyright © 2020 Massachusetts Medical Society. All rights reserved