正在加载图片...
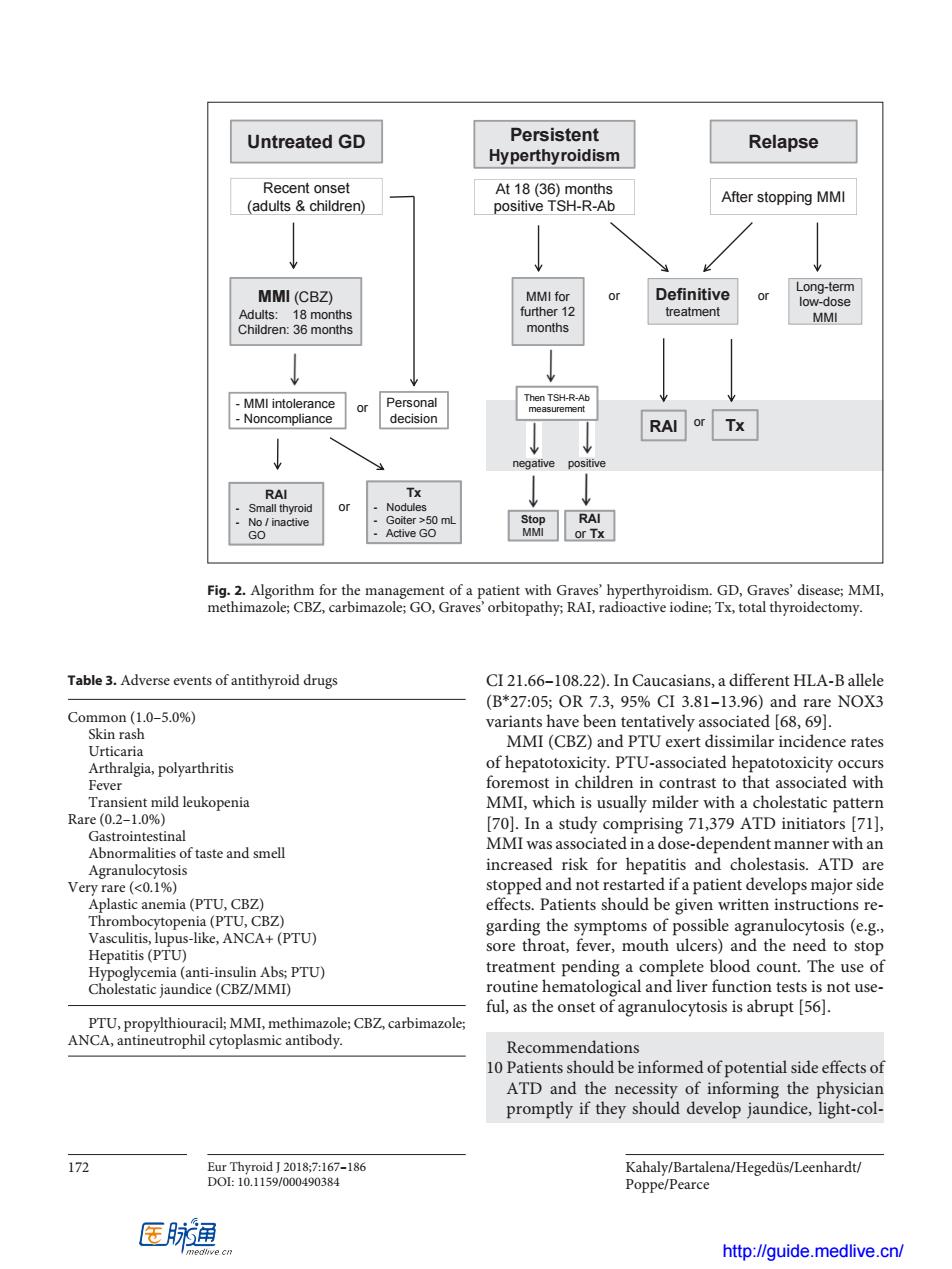
Untreated GD Persistent Relapse Hyperthyroidism () At18(36)m After stopping MMI MMI(CBZ) or Definitive or treatment RAl or Tx or MVP on Th Table3.Adverse events of antithyroid drugs CI 21.66-108.22).In Caucasians,a different HLA-Ballele (B*27:05;OR7.3,95%CI3.81-l3.96)and rare NOX3 Com Aaila,porahrits MMICBd PTUrience similar incidence rates Fever 701 In a study c ing 71.379 ATD initiato gf711 Abnormalities of taste and smell MMI was associated in a dose-dependent manner with an increased risk for hepatitis and cholestasis.ATD are stopped and not restarted ifa patient develops major side effects.Patients should be given written instructions re- er,mouth s)and the neec nd ete Recommendations 10 Patients should be informed of potential side effectsof ATD and the necessity of informing the physician promptly if they should develop jaundice,light-col- Kahaly/Bartalena/Hegeduis/Leenhardt/ Poppe/Pearce 医脉通 http://guide.medlive.cn/ Kahaly/Bartalena/Hegedüs/Leenhardt/ Poppe/Pearce 172 Eur Thyroid J 2018;7:167–186 DOI: 10.1159/000490384 CI 21.66–108.22). In Caucasians, a different HLA-B allele (B*27:05; OR 7.3, 95% CI 3.81–13.96) and rare NOX3 variants have been tentatively associated [68, 69]. MMI (CBZ) and PTU exert dissimilar incidence rates of hepatotoxicity. PTU-associated hepatotoxicity occurs foremost in children in contrast to that associated with MMI, which is usually milder with a cholestatic pattern [70]. In a study comprising 71,379 ATD initiators [71], MMI was associated in a dose-dependent manner with an increased risk for hepatitis and cholestasis. ATD are stopped and not restarted if a patient develops major side effects. Patients should be given written instructions regarding the symptoms of possible agranulocytosis (e.g., sore throat, fever, mouth ulcers) and the need to stop treatment pending a complete blood count. The use of routine hematological and liver function tests is not useful, as the onset of agranulocytosis is abrupt [56]. Recommendations 10 Patients should be informed of potential side effects of ATD and the necessity of informing the physician promptly if they should develop jaundice, light-colTable 3. Adverse events of antithyroid drugs Common (1.0–5.0%) Skin rash Urticaria Arthralgia, polyarthritis Fever Transient mild leukopenia Rare (0.2–1.0%) Gastrointestinal Abnormalities of taste and smell Agranulocytosis Very rare (<0.1%) Aplastic anemia (PTU, CBZ) Thrombocytopenia (PTU, CBZ) Vasculitis, lupus-like, ANCA+ (PTU) Hepatitis (PTU) Hypoglycemia (anti-insulin Abs; PTU) Cholestatic jaundice (CBZ/MMI) PTU, propylthiouracil; MMI, methimazole; CBZ, carbimazole; ANCA, antineutrophil cytoplasmic antibody. negative Untreated GD Persistent Hyperthyroidism Relapse MMI (CBZ) Adults: 18 months Children: 36 months - MMI intolerance - Noncompliance Tx - Nodules - Goiter ˃50 mL - Active GO MMI for further 12 months Recent onset (adults & children) At 18 (36) months positive TSH-R-Ab After stopping MMI Long-term low-dose MMI Then TSH-R-Ab measurement Definitive treatment RAI or or or or or positive Personal decision RAI - Small thyroid - No / inactive GO Stop MMI RAI or Tx Tx Fig. 2. Algorithm for the management of a patient with Graves’ hyperthyroidism. GD, Graves’ disease; MMI, methimazole; CBZ, carbimazole; GO, Graves’ orbitopathy; RAI, radioactive iodine; Tx, total thyroidectomy. http://guide.medlive.cn/