正在加载图片...
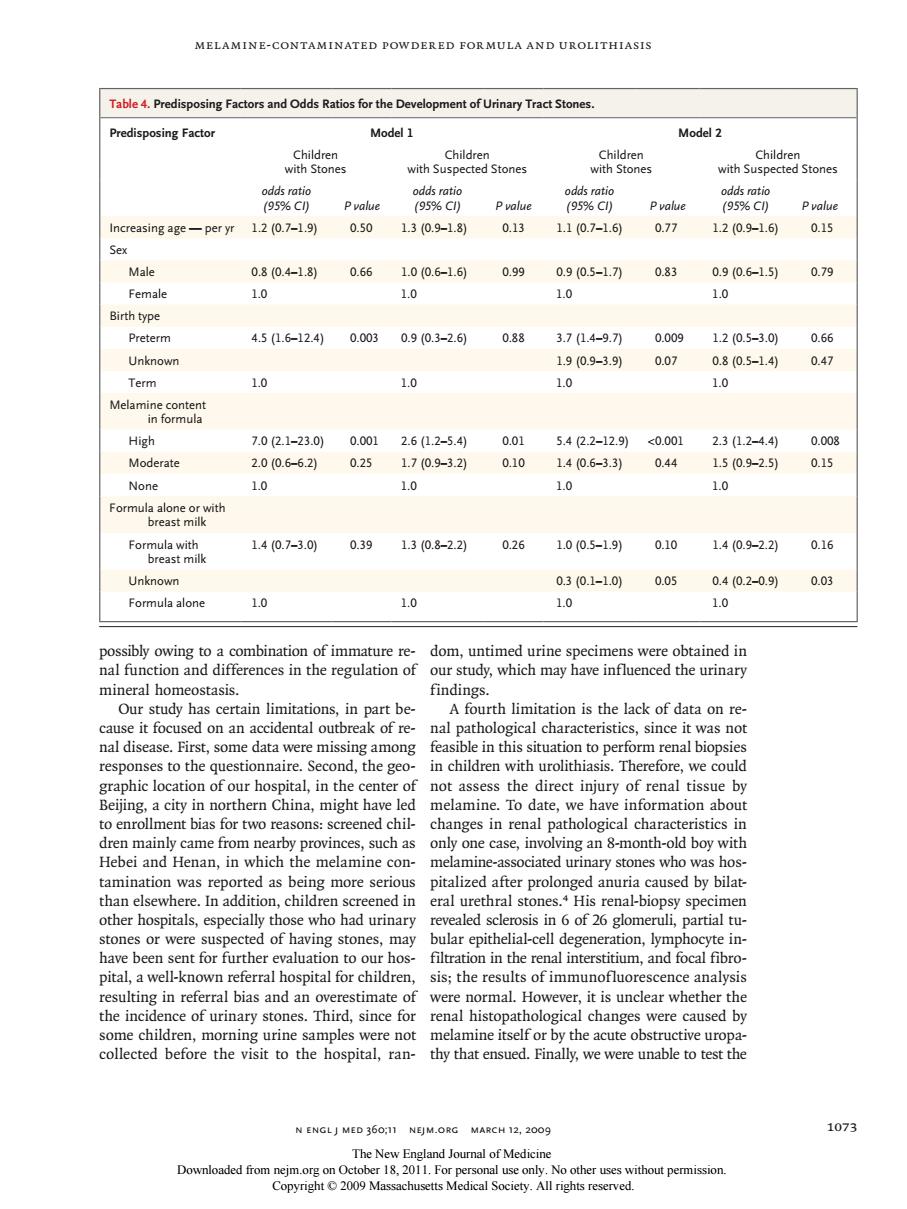
MELAMINE-CONTAMINATED POWDERED FORMULA AND UROLITHIASIS Table4.Predisposing Factors and Odds Ratios for the Development of Urinary TractStones Predisposing Factor Model 1 Model 2 Children with Su 95%cC 95%C) Pvolue 95%C) Pvalue 95%C) Pvalue Increasing age-per yr 1.20.7-19 050 1.3(0.9-1.8) 0.13 1.10.7-1.6 0.77 120.9-1.)0.15 Male 0804-1.8 0.66 1.0(0.6-1.6 0.99 0.910.5-171 0.83 0.90.6-15) 0.79 Femal 1.0 10 Birth type Preterm 4.51.6-12.400.0030.9(0.3-2.句0.88 3.7(1.4-9.70 000g 120.5-3.0 0.66 Unknown 190.9-3.9) 0.07 0.80.5-1.4)0.47 Term 1.0 1.0 1.0 1.0 High 7.0(2.1-23.010.0012.6(1.2-5.4 0.01 5.4(2.2-12.9)<0.001 23(1.2-4.4) 0.008 Moderate 2.0(0.6-6.2) 0.25170.9-32) 0101.40.6-3.3)0.44 1.50.9-2.5)0.15 None 1.0 1.0 1.0 1.0 Formula alo 1.40.7-3.00.391.3(0.8-22) 0.26 1.00.5-1.9) 0.10 1.40.9-2.2)0.16 0.30.1-1.0 005 0402-0.9 0.03 a alone 1.0 1.0 ssibly owing to a combination of immature re-dom.untimed urine specimens were obtained in nal function and differences in the regulation of our study,which may have influenced the urinary mineral homeostasis. findings. Our study has certain limitations,in part be A fourth limitation is the lack of data on re- it focused on an accidental outbreak ofre as not data were mis nd childr ital in the dire ot in to enrollment bias for two reasons:screened chil changes in renal pathological characteristics in dren mainly came from nearby provinces,such as only one case,involving an 8-month-old boy with Hebei and Henan,in which the melamine con melamine-associated urinary stones who was hos after prolonged anuria caused by bilat e.mna eral ure blopsy spe stones or w ected of hau tones ma bular epithelial-cell deg ration,ym te in have been sent for further evaluation to our hos-filtration in the renal interstitium,and focal fibro pital,a well-known referral hospital for children,sis;the results of immunofluorescence analysis resulting in referral bias and an overestimate of were normal.However,it is unclear whether the the inc l changes were caused by en,m by the acute ob naly,we were unable N ENGLJ MED 360,11 NEJM.ORG MARCH 12,2009 1073 Dowloadedom11.For pooN CegWhoutpemision Melamine-Contaminated Powdered Formula and Urolithiasis n engl j med 360;11 nejm.org march 12, 2009 1073 possibly owing to a combination of immature renal function and differences in the regulation of mineral homeostasis. Our study has certain limitations, in part because it focused on an accidental outbreak of renal disease. First, some data were missing among responses to the questionnaire. Second, the geographic location of our hospital, in the center of Beijing, a city in northern China, might have led to enrollment bias for two reasons: screened children mainly came from nearby provinces, such as Hebei and Henan, in which the melamine contamination was reported as being more serious than elsewhere. In addition, children screened in other hospitals, especially those who had urinary stones or were suspected of having stones, may have been sent for further evaluation to our hospital, a well-known referral hospital for children, resulting in referral bias and an overestimate of the incidence of urinary stones. Third, since for some children, morning urine samples were not collected before the visit to the hospital, random, untimed urine specimens were obtained in our study, which may have influenced the urinary findings. A fourth limitation is the lack of data on renal pathological characteristics, since it was not feasible in this situation to perform renal biopsies in children with urolithiasis. Therefore, we could not assess the direct injury of renal tissue by melamine. To date, we have information about changes in renal pathological characteristics in only one case, involving an 8-month-old boy with melamine-associated urinary stones who was hospitalized after prolonged anuria caused by bilateral urethral stones.4 His renal-biopsy specimen revealed sclerosis in 6 of 26 glomeruli, partial tubular epithelial-cell degeneration, lymphocyte infiltration in the renal interstitium, and focal fibrosis; the results of immunofluorescence analysis were normal. However, it is unclear whether the renal histopathological changes were caused by melamine itself or by the acute obstructive uropathy that ensued. Finally, we were unable to test the Table 4. Predisposing Factors and Odds Ratios for the Development of Urinary Tract Stones. Predisposing Factor Model 1 Model 2 Children with Stones Children with Suspected Stones Children with Stones Children with Suspected Stones odds ratio (95% CI) P value odds ratio (95% CI) P value odds ratio (95% CI) P value odds ratio (95% CI) P value Increasing age — per yr 1.2 (0.7–1.9) 0.50 1.3 (0.9–1.8) 0.13 1.1 (0.7–1.6) 0.77 1.2 (0.9–1.6) 0.15 Sex Male 0.8 (0.4–1.8) 0.66 1.0 (0.6–1.6) 0.99 0.9 (0.5–1.7) 0.83 0.9 (0.6–1.5) 0.79 Female 1.0 1.0 1.0 1.0 Birth type Preterm 4.5 (1.6–12.4) 0.003 0.9 (0.3–2.6) 0.88 3.7 (1.4–9.7) 0.009 1.2 (0.5–3.0) 0.66 Unknown 1.9 (0.9–3.9) 0.07 0.8 (0.5–1.4) 0.47 Term 1.0 1.0 1.0 1.0 Melamine content in formula High 7.0 (2.1–23.0) 0.001 2.6 (1.2–5.4) 0.01 5.4 (2.2–12.9) <0.001 2.3 (1.2–4.4) 0.008 Moderate 2.0 (0.6–6.2) 0.25 1.7 (0.9–3.2) 0.10 1.4 (0.6–3.3) 0.44 1.5 (0.9–2.5) 0.15 None 1.0 1.0 1.0 1.0 Formula alone or with breast milk Formula with breast milk 1.4 (0.7–3.0) 0.39 1.3 (0.8–2.2) 0.26 1.0 (0.5–1.9) 0.10 1.4 (0.9–2.2) 0.16 Unknown 0.3 (0.1–1.0) 0.05 0.4 (0.2–0.9) 0.03 Formula alone 1.0 1.0 1.0 1.0 The New England Journal of Medicine Downloaded from nejm.org on October 18, 2011. For personal use only. No other uses without permission. Copyright © 2009 Massachusetts Medical Society. All rights reserved