正在加载图片...
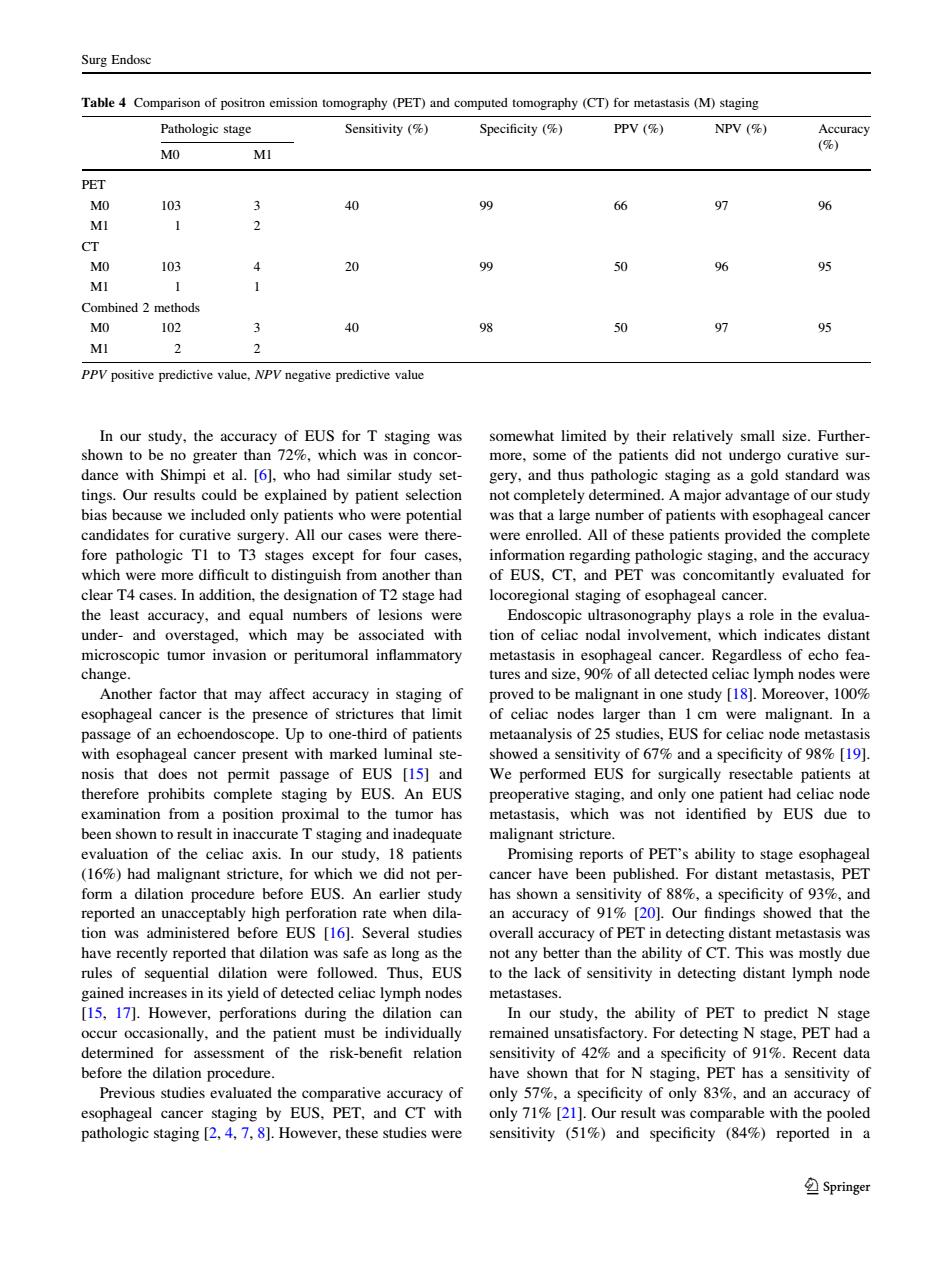
Surg Endose Table Comparison of (PETand computed (CT or metastasis (M)san Pathologic stage Sensitivity (% Specificity ( PPV ( NPV (% MO PET MO 103 40 96 MI 103 20 99 96 95 ned m 102 40 97 MI PPV positive predictive value,NPV negative predictive value In our study.the of FUS for T sta shown to be n s did no urativ dance with Shimpi et al.[6],who had similar study set- gery,and thus pathologic staging as a gold standard was tings.Our results could be explained by patient selection not completely determined.A major advantage of our study bias because we included only patients who were potential was that a large number of patients with esophageal cancer andida ere there re enrolle All of th the complete slear Ta cases In addition the d tion of T2 stage had the least accuracy.and equal numbers of lesions were under-and overstaged,which may be associated with tion of celiac nodal involvement,which indicates distant microscopic tumor invasion or peritumoral inflammatory cancer.Regardless of echo tea change r factor that nay affe eofuracy in s dy than 1 er .Up to one-third of patients metaanalysis of 25 studies.EUS for celiac node metastasis with esophageal cancer present with marked luminal ste- showed a sensitivity of 67 and a specificity of9%19] nosis that does not permit passage of EUS [15]and We performed EUS for surgically resectable patients at therefore prohibits complete staging by EUS An EUS hac node a position proxim e tumor has pmeeTrairesthene.andoo8eientNhag met was not identified by EUS due to agndy 18 of PET's ability to st had malignant stricture.for which we did no form a dilation procedure before EUS.An earlier study has shown a sensit vity of 88.a s pecificity of93%and an accuracy Our findings showed that the ion was dminis verall accuracy of P lete ng dis tant metasta EUS than the ed in s in its vield of detected celiac i h n [15 171 However perforations during the dilation can In our study.the ability of PET to predict N stage occur occasionally.and the patient must be individually remained unsatisfactory.For detecting N stage.PET had a determined for assessment of the risk-benefit relation sensitivity of 42%and a specificity of 91%.Recent data before the dilation procedure have shown that for N staging.PET has a sensitivity of studies evalu nd Cr mg2.4.781H weve udi (51% reported in Springer In our study, the accuracy of EUS for T staging was shown to be no greater than 72%, which was in concordance with Shimpi et al. [6], who had similar study settings. Our results could be explained by patient selection bias because we included only patients who were potential candidates for curative surgery. All our cases were therefore pathologic T1 to T3 stages except for four cases, which were more difficult to distinguish from another than clear T4 cases. In addition, the designation of T2 stage had the least accuracy, and equal numbers of lesions were under- and overstaged, which may be associated with microscopic tumor invasion or peritumoral inflammatory change. Another factor that may affect accuracy in staging of esophageal cancer is the presence of strictures that limit passage of an echoendoscope. Up to one-third of patients with esophageal cancer present with marked luminal stenosis that does not permit passage of EUS [15] and therefore prohibits complete staging by EUS. An EUS examination from a position proximal to the tumor has been shown to result in inaccurate T staging and inadequate evaluation of the celiac axis. In our study, 18 patients (16%) had malignant stricture, for which we did not perform a dilation procedure before EUS. An earlier study reported an unacceptably high perforation rate when dilation was administered before EUS [16]. Several studies have recently reported that dilation was safe as long as the rules of sequential dilation were followed. Thus, EUS gained increases in its yield of detected celiac lymph nodes [15, 17]. However, perforations during the dilation can occur occasionally, and the patient must be individually determined for assessment of the risk-benefit relation before the dilation procedure. Previous studies evaluated the comparative accuracy of esophageal cancer staging by EUS, PET, and CT with pathologic staging [2, 4, 7, 8]. However, these studies were somewhat limited by their relatively small size. Furthermore, some of the patients did not undergo curative surgery, and thus pathologic staging as a gold standard was not completely determined. A major advantage of our study was that a large number of patients with esophageal cancer were enrolled. All of these patients provided the complete information regarding pathologic staging, and the accuracy of EUS, CT, and PET was concomitantly evaluated for locoregional staging of esophageal cancer. Endoscopic ultrasonography plays a role in the evaluation of celiac nodal involvement, which indicates distant metastasis in esophageal cancer. Regardless of echo features and size, 90% of all detected celiac lymph nodes were proved to be malignant in one study [18]. Moreover, 100% of celiac nodes larger than 1 cm were malignant. In a metaanalysis of 25 studies, EUS for celiac node metastasis showed a sensitivity of 67% and a specificity of 98% [19]. We performed EUS for surgically resectable patients at preoperative staging, and only one patient had celiac node metastasis, which was not identified by EUS due to malignant stricture. Promising reports of PET’s ability to stage esophageal cancer have been published. For distant metastasis, PET has shown a sensitivity of 88%, a specificity of 93%, and an accuracy of 91% [20]. Our findings showed that the overall accuracy of PET in detecting distant metastasis was not any better than the ability of CT. This was mostly due to the lack of sensitivity in detecting distant lymph node metastases. In our study, the ability of PET to predict N stage remained unsatisfactory. For detecting N stage, PET had a sensitivity of 42% and a specificity of 91%. Recent data have shown that for N staging, PET has a sensitivity of only 57%, a specificity of only 83%, and an accuracy of only 71% [21]. Our result was comparable with the pooled sensitivity (51%) and specificity (84%) reported in a Table 4 Comparison of positron emission tomography (PET) and computed tomography (CT) for metastasis (M) staging Pathologic stage Sensitivity (%) Specificity (%) PPV (%) NPV (%) Accuracy (%) M0 M1 PET M0 103 3 40 99 66 97 96 M1 1 2 CT M0 103 4 20 99 50 96 95 M1 1 1 Combined 2 methods M0 102 3 40 98 50 97 95 M1 2 2 PPV positive predictive value, NPV negative predictive value Surg Endosc 123